Locations:

Confounding symptoms and a complex medical history prove diagnostically challenging

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4307bfbc-5329-4e52-a9e5-d8e214b758f6/purple-toes-case-study-1629904372)
Foot examination
This article is reprinted without references from the Cleveland Clinic Journal of Medicine (December 2024, 91 (12) 735-741; doi: 10.3949/ccjm.91a.24064.) The open-access and fully referenced original article is available at ccjm.org/content/91/12/735.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
By Baila R. Elkin, MD and Megan McGervey, MD
A 74-year-old woman presented to the hospital from the podiatry clinic for evaluation of bilateral foot pain and purple toes. She had a history of Janus kinase (JAK) 2 V617F–positive polycythemia vera, Raynaud syndrome, gastroesophageal reflux disease, prior breast cancer and thyroid cancer, hypertension, and deep vein thrombosis and pulmonary embolism.
The patient's polycythemia vera had been treated with aspirin, which was discontinued due to stomach upset, and hydroxyurea, which was also recently discontinued. She was started on apixaban following her deep vein thrombosis and pulmonary embolism episode and was still taking it at the time she presented.
The patient reported that her symptoms began about 5 months earlier. At that time, she experienced intermittent burning foot pain, worsened by prolonged sitting and standing. She developed painful ulcers on her right hallux, described as “black dots” that expanded, and later developed additional ulcers on her left lateral ankle and right anterior shin. The ulcer on her left ankle was biopsied and found to be consistent with livedoid vasculopathy.
She was started on pentoxifylline and nifedipine, and hydroxyurea was discontinued due to concern that it was contributing to her ulcerations. The ulcers initially improved with wound care. However, about 3 weeks before her current presentation, her toes started to become purple, with persistent “stinging” pain that improved somewhat with warmth and elevation.
Advertisement
On presentation, violaceous discoloration of both feet was noted, with necrotic tissue present distally (Figure 1). Her feet were cold to the touch, with palpable dorsalis pedis pulses bilaterally and intact sensation and strength. Cardiac examination was unremarkable, without murmurs, rubs, or gallops. Palpation of her abdomen did not reveal splenomegaly. No joint swelling, erythema, or tenderness to palpation was present.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c1e7d0fd-a65f-4172-ad91-f90be6daf623/purple-toes-case-study-inset-1)
(Figure 1) Violaceous discoloration of patient’s toes on presentation
1. What is the most likely diagnosis?
The differential diagnosis for purple digits is broad. In a hemodynamically stable patient, emergent etiologies include acute limb ischemia, embolic microthrombi, purpura fulminans, and catastrophic antiphospholipid syndrome (APS). Purple digits stem from abnormal blood flow, which can have various causes. These include microembolisms from upstream clots, large aneurysms, peripheral vascular disease, vasospasm, vasculitis and pseudovasculitis, thrombosis or mechanical obstruction, cryoglobulinemia, myeloproliferative syndromes, and hypercoagulability secondary to malignancies or hypercoagulable syndromes.
Laboratory test results were notable for hyponatremia to 126 mmol/L (reference range 132–148) and hypokalemia to 3.6 mmol/L (3.7–5.1). A pulse volume recording showing an ankle-brachial index (i.e., the systolic blood pressure in the ankle divided by the higher of the systolic pressures in the 2 arms) of 1.08 on the right and 1.02 on the left (1–1.4). A complete blood cell count without differential showed the following:
Advertisement
A differential the next day showed the following: white blood cell count 36 × 109/L, with 89% neutrophils (42–75), 4% lymphocytes (16–52), 1% monocytes (1–11), 2% eosinophils (0–7), and 1% basophils (0–4).
A partial workup for thrombophilia had been done when the patient developed lower-extremity ulcers, but full lupus anticoagulant testing was not completed at that time.
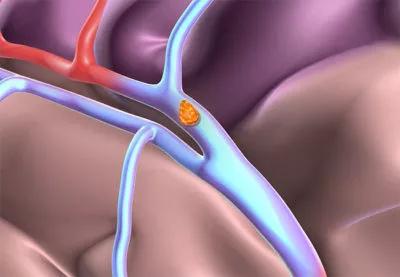
To evaluate for neoplastic syndrome, a computed tomography imaging of the chest, abdomen, and pelvis was obtained and showed an 8-mm thrombus (Figure 2).

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/87b376a2-a551-49aa-a014-8c3f8ee78f51/purple-toes-case-study-inset-2)
(Figure 2) CT scan showing aortic thrombus
2. What aspect of this patient’s history or treatment would prevent full lupus anticoagulant testing?
APS is an autoimmune condition in which the presence of antiphospholipid antibodies leads to thrombosis or obstetric complications. Clinical criteria include the presence of arterial, venous, or small-vessel thrombosis or obstetric complications, while laboratory criteria include the presence of antiphospholipid antibodies in plasma, namely lupus anticoagulant, anticardiolipin, or anti–beta-2-glycoprotein 1 antibodies.
Full lupus anticoagulant testing could not be completed in this patient because she was taking apixaban. DOACs can affect APS laboratory assays, causing both false-positive and false-negative lupus anticoagulant findings, and different DOACs affect the assays differently.
Other anticoagulants can also interfere with testing, but established neutralizers for heparin included in many reagents for the dilute Russell’s viper venom time, a common test for lupus anticoagulant, help mitigate this. Several strategies have been proposed to evaluate patients on DOACs for APS, including pausing DOAC, DOAC antagonists, and DOAC removal from the specimen, although these are not available in many laboratories.
Advertisement
3. What is the most likely location of this patient’s thrombus?
The presence of bilateral symptoms from thromboembolic disease implies either bilateral thrombi or a central arterial thromboembolic source. Venous thrombi would propagate towards the heart, not distally. The central arterial source is most commonly the heart, where structural or functional abnormalities can cause clot to form, and thus an echocardiogram is an essential part of the evaluation for arterial thrombi, even when, as in this patient, the cardiac examination revealed no murmurs or other abnormalities.
Thrombi within or proximal to the heart can embolize anywhere in the body, while more distal thrombi have fewer potential locations. A thrombus in the carotid arteries would be more likely to embolize to the brain than to the lower extremities. A rare but serious cause of peripheral embolism is mural thrombus in the aorta.
4. What is the preferred anticoagulant agent for APS?
Two factors in the current presentation could disrupt testing: use of heparin and the presence of active thrombosis. While heparin can be neutralized by specific reagents during lupus anticoagulant testing, heparin levels can exceed the neutralizing ability, and these reagents are not usually present in activated partial thromboplastin time reagents. Thus, results obtained in this clinical context should be interpreted with caution and repeated in the coming weeks, as recommended by vascular medicine.
Advertisement
APS is associated with a characteristic netlike “livedo” rash, which can be further classified into livedo reticularis and livedo racemosa. Both are caused by reduced blood flow, but livedo racemosa is more widely distributed on the trunk and the limbs, is irregular and broken in shape, has abnormal histopathology findings, is always pathologic, and is associated with APS and several other diseases. Although this patient’s skin findings were not characteristic of livedo, with violaceous digits rather than a net-like violaceous pattern, her APS adds further evidence for increased thrombotic risk.
Vascular medicine recommended an intravenous heparin drip for 72 hours with a target activated partial thromboplastin time of 53 to 78 seconds, with a plan to transition to therapeutic enoxaparin 1 mg/kg twice daily for 4 weeks, followed by a bridge to warfarin with a target INR of 2 to 3 and clopidogrel. The patient’s burning bilateral foot pain continued despite the heparin therapy. She underwent aortography with suction thrombectomy of her infrarenal aortic thrombus, after which her pain improved, and she was discharged.
Advertisement

Aim is for use with clinician oversight to make screening safer and more efficient

Findings help close the knowledge gap around VTE practice patterns

Conservative treatments were ineffective for 29-year-old with chronic heel pain

Oral anticoagulants may be beneficial but need to be balanced against bleeding risks
Higher complete reperfusion rate seen with tenecteplase vs. alteplase in single-center study of stroke with LVO

The relationship between MTHFR variants and thrombosis risk is a complex issue, but current evidence points to no association between the most common variants and an elevated risk

Large cohort study finds significant effect in men and nonsmokers
Clinicians highlight the need to educate patients about warning signs