Locations:

CAR T-cell therapy may offer reason for optimism that those with SLE can experience improvement in quality of life.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0cf3ddff-3cdd-422d-ad22-ae224bfaa6de/RHE_5631008_03-06-25_1014_AMO)
Dr. Littlejohn with patient in clinic
Emily Littlejohn, DO, MPH
For four years, a woman in her 20s with systemic lupus erythematosus (SLE) experienced a host of symptoms so severe that she was unable to perform basic activities of daily living: work, family celebrations, sports — even simply driving to the store.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
That was until March 2023 at Cleveland Clinic, when she became the second participant in an international phase 1 clinical trial of chimeric antigen receptor (CAR) T-cell treatment for severe, refractory lupus. Six months after treatment, she was in drug-free remission and had returned to those activities she enjoyed before her diagnosis, and more.
As clinicians and scientists investigating CAR T-cell therapy for SLE and other autoimmune diseases, we temper hope with an understanding of the need for more research and data. Rigorous clinical trials and lab metrics are necessary to measure safety, efficacy and the longevity of this therapy.
As this patient’s experience underscores, however, it is important to acknowledge patient-reported improvements in symptoms such as fatigue, depression and brain fog that are hard to measure with traditional disease activity tools.
Background
In February 2019, JG was diagnosed with autoimmune hepatitis (lupus hepatitis). She was placed on daily azathioprine and tacrolimus and was feeling well until November 2019, when she was found to have proteinuria. Cleveland Clinic nephrologists examined her and performed a renal biopsy was performed; it showed membranous glomerulonephritis with mesangial and subepithelial electron-dense deposits with foot process effacement, consistent with class V lupus nephritis. She was then switched to mycophenolate mofetil from azathioprine.
Around this time, the patient began to report chest pain and difficulty breathing. A chest CT revealed an acute pulmonary embolism causing small infarct and small left pleural effusion. CT also showed bilateral axillary/subpectoral lymphadenopathy. A left axillary lymph node biopsy revealed no evidence of a metastatic neoplasm or granulomatous inflammation. Given the presence of antiphospholipid antibodies, the patient was placed on warfarin.
Advertisement
Over time, she developed severe hip pain, and an MRI showed bilateral avascular necrosis, a known complication of SLE. Over the course of six months, both hips were replaced. Due to ongoing joint pain and diffuse adenopathy, the patient was eventually given belimumab subcutaneous weekly injections and, later, rituximab infusions, with only some decrease in joint pain.
Unfortunately, she continued to experience the fatigue and brain fog that had caused her to stop work and other activities, such as traveling and working out, for more than four years.
In December 2023, the patient received her last rituximab infusion. In March 2024, she was enrolled in a phase 1 CAR T-cell therapy clinical trial for severe, refractory lupus. She experienced no cytokine release syndrome or immune effector cell-associated neurotoxicity syndrome during or after her CAR T-cell therapy infusion. At nine months out from CAR T-cell therapy, the patient remained in drug-free remission and had returned to social activities. Seeing her in office, she endorsed less fatigue and an overall sense of well-being and improved mood — something not capturable or reportable by measures of disease activity in SLE, but life-changing for this patient. She was excited to be planning a vacation cruise and coming off disability status to return to work.
Takeaways
For many individuals with lupus, the toll of the disease extends beyond the difficulties of managing organ damage and physical symptoms such as joint pain, rash or alopecia. Those with lupus also suffer from chronic fatigue, brain fog and depression, symptoms that are difficult to measure but significantly impair overall sense of well-being. CAR T-cell therapy not only offers the chance to put severe, refractory lupus into a drug-free remission, but is providing reason for optimism that those with SLE may experience improvement in quality of life.
Advertisement
Advertisement

Drug-free remission holds more than a year after treatment
Advancements lead to a new trial involving autoimmune disease

Lupus Clinic providers collaborate to advance treatment and understanding

A review of expanding options that hold new promise

Disease associated with higher risks for maternal and fetal morbidities
Early data show risk is 73% higher in patients with lupus, 40% higher in patients with rheumatoid arthritis

Cleveland Clinic’s Rheumatic Lung Disease program treats patients with complex conditions
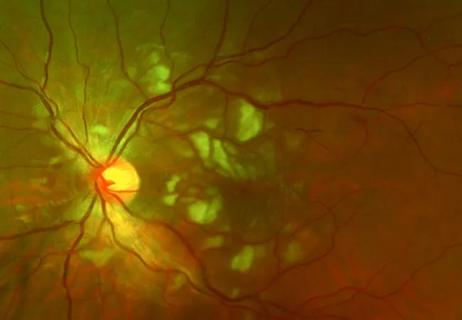
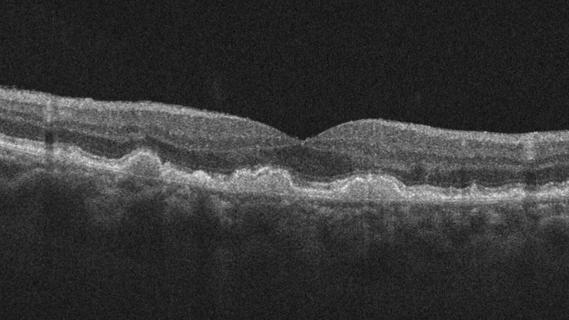
Good visual recovery and retinal reperfusion after prompt diagnosis and intensive therapy