Locations:

Identifies weak spots in the cornea before shape change occurs

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6cea4ec7-b6ed-4a43-abde-61a2e35fb9ad/detecting-subclinical-keratoconus)
Target with areas marked in different colors: blue, green and yellow
For the first time, researchers have shown that Brillouin microscopy can detect keratoconus in its early stages, before it becomes clinically evident.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
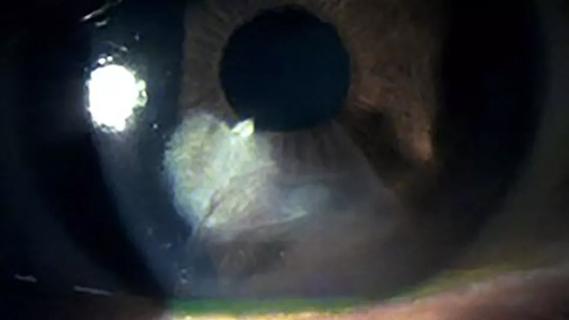
Keratoconus is fairly easy to diagnose in its later stages, when the natural curve of the cornea bulges into a cone shape and causes vision loss. Treatments like corneal cross-linking can reinforce the cornea and stop the progression of vision loss, but they can’t restore vision. That’s why earlier detection of keratoconus (and the corneal weakening that precedes it) would be better for patients — so treatment can begin sooner, and vision loss can be prevented.
To screen for keratoconus, ophthalmology clinics routinely use Scheimpflug tomography, a tool that uses 3D imaging to assess corneal curvature.
“When there aren’t overt signs of keratoconus, however, Scheimpflug imaging can be inconclusive,” says J. Bradley Randleman, MD, a cornea and refractive surgery specialist at Cleveland Clinic Cole Eye Institute. “We can get the metrics — like front-surface curvature, front-surface elevation, back-surface elevation and corneal thickness — but these data can be contradictory.”
In recent research, Dr. Randleman and colleagues studied a completely different method of evaluating corneal health: Brillouin microscopy. This method involves shooting beams of light into specific areas of the cornea. Shifts in light frequency indicate the stiffness and strength of corneal tissue in those spots.
Results of the study, published in Ophthalmology, indicate that motion-tracking Brillouin microscopy can identify weak spots in the cornea even before the telltale shape change occurs in keratoconus.
Advertisement
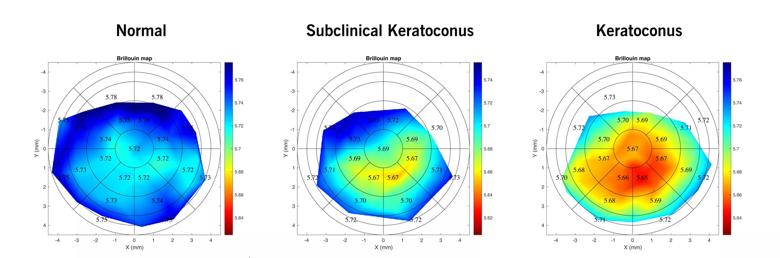
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/195a52f5-c0d6-4bea-9187-70115b67ab34/detecting-subclinical-keratoconus-inset)
Brillouin map composite
The researchers studied 15 healthy eyes and 15 eyes with suspected subclinical keratoconus (those with subtle but inconclusive findings from Scheimpflug tomography). All patients were evaluated with Scheimpflug tomography and Brillouin microscopy, which was conducted with a custom-built motion-tracking microscope.
“The motion-tracking device that we developed at Cleveland Clinic uses optical coherence tomography (OCT), so we can see where we are in three dimensions,” explains Dr. Randleman, lead author of the study.
An earlier study reported that the periphery of keratoconic corneas is often as strong as in healthy corneas. So, the new study focused on the region known to be different: more central values within the anterior third of the cornea, including the plateau region.
In that area, motion-tracking Brillouin microscopy recorded significant differences between healthy eyes and eyes with subclinical keratoconus for both mean and minimum values. Each Brillouin metric evaluated fully differentiated between keratoconic and healthy corneas (area under the curve [AUC] 1.0).
“Brillouin imaging reports focal data, the stiffness of a precise spot in the cornea,” says Dr. Randleman. “Scheimpflug imaging reports morphology [shape], not stiffness; and other devices widely used for keratoconus screening report global properties of a cornea, the overall corneal stiffness.”
That’s an important distinction because current data indicate that keratoconus starts as a focal weakness. As the weakness at one spot progresses, it becomes easier to detect with a general screening of the cornea.
Advertisement
“All suspected keratoconic corneas in this study had some kind of focal weakening that was easy to identify and useful for differentiating from healthy corneas,” says Dr. Randleman.
In the study, motion-tracking Brillouin microscopy outperformed Scheimpflug tomography in detecting subclinical keratoconus.
However, the study also identified the Scheimpflug metrics most sensitive for differentiating between keratoconic and healthy corneas. Those included: keratoconus index (AUC 0.91), inferior-superior value (AUC 0.89) and index of vertical asymmetry (AUC 0.88).
Other Scheimpflug metrics were not as sensitive for detecting keratoconus. Those included: maximum keratometry, thinnest corneal thickness, Belin/Ambrósio display total deviation and Ambrósio relational thickness.
“These findings may be most helpful to ophthalmologists in the near term, while motion-tracking Brillouin microscopy isn’t commercially available to ophthalmology clinics,” says Dr. Randleman. “We will continue to test and develop our device. Our goal is to make motion-tracking Brillouin microscopy rapid, automated and reproducible.”
Advertisement
Advertisement

Motion-tracking Brillouin microscopy pinpoints corneal weakness in the anterior stroma

Study reveals more about the pathophysiology of Salzmann’s nodular degeneration
Studies continue to indicate effectiveness and safety

Novel use of tPA reduces fibrin response in the eye

Researcher gives guidance for clinical trials

How computational tools and personalized biomechanics can improve keratoconus detection, ectasia risk assessment and surgical outcomes

Untreated seropositive erosive RA led to peripheral ulcerative keratitis

The drug does not provide lasting disease control for most patients