Locations:

Quantitative imaging adds diagnostic value beyond 3T MRI in nearly half of patients
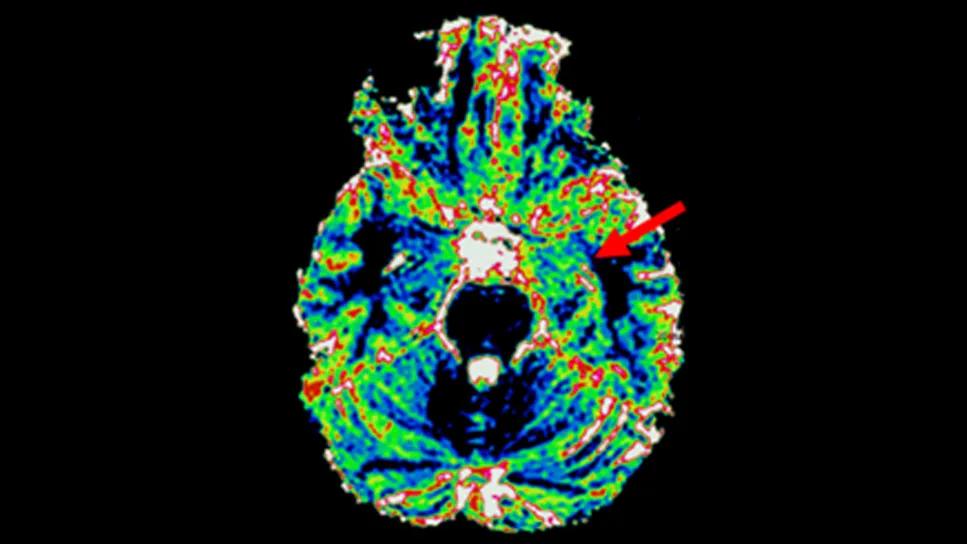
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4fcaae76-93fb-484a-a9b5-5bf874820cee/brain-scan-mr-fingerprinting-in-epilepsy)
colorful brain scan with a red arrow pointing to a spot on right side
New research from Cleveland Clinic shows that a novel imaging paradigm, magnetic resonance fingerprinting (MRF), provides significant diagnostic advantages for patients with medically refractory epilepsy.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In a retrospective analysis of 100 presurgical cases, investigators found that MRF offered additional radiologic insights beyond conventional 3T MRI in nearly half of the patients. The findings, published in Epilepsia, suggest that quantitative tissue mapping may soon become an essential adjunct in the localization of difficult-to-detect seizure origins.
“We conducted the first large-scale study of MRF in patients undergoing evaluation for epilepsy surgery, analyzing 100 cases, the largest cohort to date,” says senior author Irene Wang, PhD, Research Director, Cleveland Clinic Epilepsy Center. “We found that MRF improved the ability to detect and clearly define subtle brain abnormalities, particularly in challenging epilepsy subtypes. These findings lay the foundation for integrating MRF into routine clinical care.”
While structural MRI remains the cornerstone of epilepsy evaluation, its qualitative nature presents some challenges. Standard sequences, such as T1-weighted or FLAIR images, rely on relative signal intensities that can vary based on scanner hardware, acquisition settings and patient positioning. Additionally, subtle magnetic field irregularities, known as inhomogeneity, can create shading artifacts that mask true pathology or suggest abnormalities where none exist.
These limitations can be critical for surgeons, as clear identification of a lesion is among the strongest predictors of successful epilepsy surgery outcomes. Despite this fact, many epilepsy cases are deemed “nonlesional” based on initial imaging reports.
Advertisement
In contrast, MRF is an advanced imaging technique that generates detailed, quantitative maps of brain tissue in a single scan, providing information beyond what standard MRI can offer. Specifically, it replaces the qualitative weighting of traditional MRI with absolute quantitative measures of intrinsic tissue properties, such as T1 and T2 relaxation times.
“Cleveland Clinic’s Epilepsy Center has been an internationally recognized pioneer in translating MRF from research into clinical applications,” notes the new study’s first author, Maksim Parfyonov, MD, a staff pediatric epileptologist in the Epilepsy Center. “This investigation is our largest evaluation of that clinical application to date.”
The retrospective study examined details of 100 patients who underwent presurgical evaluation at Cleveland Clinic’s Epilepsy Center between 2017 and 2024. The researchers compared findings from standard 3T MRI clinical protocols with 10-minute, high-resolution 3D MRF acquisitions that simultaneously generated T1, T2 and gray/white matter fraction maps.
The findings underscored the high radiological yield of MRF, which provided additional diagnostic value in 46% of the patient cohort. Among the 32 patients whose initial conventional MRI reports were negative, MRF identified abnormalities or supplied new insights in 38% of cases.
Benefits were categorized into several major areas:
Advertisement
Figures 1 and 2 present representative comparative MRF and conventional MRI findings from two patients.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6425085f-6fcb-43f5-927a-08775a889207/brain-scans-mr-fingerprinting-epilepsy-inset-1)
Figure 1. Images from a 30-year-old woman with left mesial temporal epilepsy who became seizure-free after SEEG-guided surgery. Conventional MRI was completely nonlesional. SEEG showed left mesial temporal onset. MRF T1 shows increased signal in the left mesial temporal region (arrow), which was concordant with SEEG onset and resection.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/978126e1-be0f-4caa-b6b7-90325f829a7f/brain-scans-mr-fingerprinting-epilepsy-inset-2)
Figure 2. MRF reveals a more extensive epileptogenic lesion in a 27-year-old woman with mild malformation of cortical development with oligodendroglial hyperplasia and epilepsy (MOGHE) who became seizure-free after resection. Conventional MRI was initially read as negative, with only a subtle right posterolateral frontal abnormality suspected. MRF T1 and white-matter (WM) fraction maps better delineated lesion extent and abnormal white-matter architecture.
The diagnostic impact of MRF was especially striking in specific histologic subgroups. For patients with focal cortical dysplasia (FCD), the yield varied significantly by subtype. While FCD type IIb is often visible on standard MRI, FCD type IIa is more subtle.
Notably, MRF added diagnostic value in 78% of FCD type IIa cases compared with only 17% of type IIb cases. Similarly, the modality proved highly effective for detecting periventricular nodular heterotopia, providing additional information in 88% of such cases.
“MRF proved especially valuable in defining subtle brain abnormalities, particularly in conditions such as periventricular nodular heterotopia and FCD type IIa, which are often difficult to identify but critically important for surgical planning,” Dr. Parfyonov observes.
The success of MRF stems from its biophysical basis, the authors note. By matching acquired signal patterns against a vast dictionary of simulated tissue signatures, the system generates maps independent of external variables. For example, hypomyelination, which is a common feature in many epileptogenic lesions, lengthens T1 relaxation times. The study showed that, among MRF-generated images, T1 maps were generally more helpful than T2 maps, as T1 provided superior diagnostic utility in 32 patients whereas T2 was more valuable in only nine patients.
Another distinctive advantage of the 3D MRF protocol used at Cleveland Clinic is its inclusion of what the authors describe as integrated B1 mapping. This allows the system to correct for field inhomogeneities that often plague standard imaging, especially in the inferior temporal lobes where many seizure foci originate. The result is a “flatter” image that gives more confidence that a regional signal change represents a real tissue difference rather than a technical artifact.
Advertisement
To facilitate use in a busy clinical environment, the researchers reviewed the quantitative maps within their standard picture archiving and communication system. They used custom colorized scales to maximize the dynamic range, making it easier to detect subtle features like blurring at the gray-white matter junction.
The authors note that despite the promise of MRF, challenges to its widespread adoption remain. Reconstructing complex MRF maps requires significant computational power, large data dictionaries and specialized expertise. Also, current MRF sequences lack the fluid suppression found in traditional FLAIR imaging and can sometimes limit the ability to assess lesions near the interface of brain and bone due to higher variability in skull signal. However, rapid technical advances are increasingly likely to mitigate these challenges.
With recent FDA clearance of MRF for initial implementation, the researchers say the path toward routine clinical use is becoming clearer. “The case for integrating MRF into routine clinical care is growing, with the goal of improving diagnostic accuracy, guiding more precise surgical treatment and ultimately enhancing outcomes for patients with epilepsy,” Dr. Wang concludes.
Advertisement
Advertisement

Two studies from Cleveland Clinic may help advance the technology toward broader clinical use

Researchers pair quantitative imaging with AI to improve surgical outcomes in nonlesional epilepsy

Free portal helps researchers classify and share data using the IC-CoDE framework

Data-driven segmentation approach shows promise for seizure characterization with utility for clinical decision making

Early identification of temporal encephaloceles can improve surgical decision-making

Insights from one of the first studies of invasive monitoring in the rare form of focal cortical dysplasia

Overcoming barriers to implementing clinical trials

An expert’s take on evolving challenges, treatments and responsibilities through early adulthood