Locations:

Treatments differ widely in these mimics
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8918d649-8d04-42db-9c00-9b43b171ef62/18-RHE-1123-Hajj-Ali-Hero-Image-650x450pxl_jpg)
18-RHE-1123-Hajj-Ali-Hero-Image-650x450pxl
By Rula Hajj-Ali, MD, and Leonard Calabrese, DO
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Distinguishing between reversible cerebral vasoconstriction syndrome (RCVS) and primary angiitis of the central nervous system (PACNS) is critical because the treatment protocol is so vastly different. Misdiagnosing PACNS as RCVS can deprive a patient of medications that prolong survival and improve outcomes. Prognosis improves greatly with proper treatment. We offer a brief overview of differences in management techniques below. See these posts for differences in clinical presentation and imaging and test results.
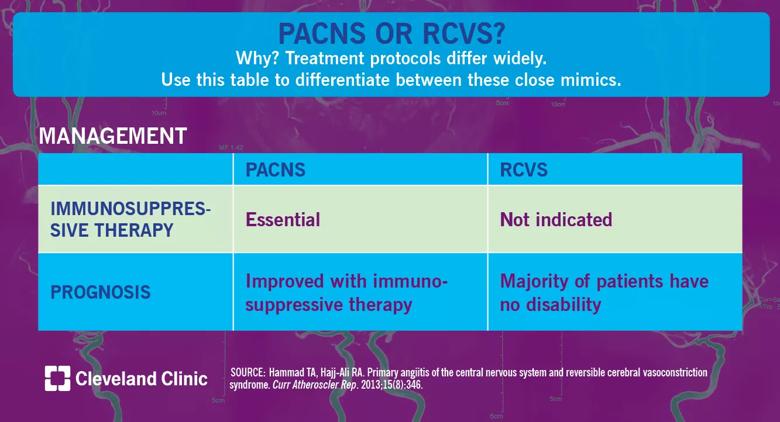
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f088a773-4051-4470-a0d3-73877cfb127e/18-RHE-1077-PACNS-or-RCVS-Visual-Abstract-1200x650pxl_04_10_2018_03b_jpg)
Before the advent of immunosuppressive therapies, the prognosis for PACNS was dismal. Survival improves with aggressive therapy. The use of immunosuppressive therapy in not indicated in RCVS, as the pathogenetic mechanisms are related to vasospasm and not inflammation; calcium channel blockers are commonly used to control headaches.
We have recently elucidated functional capabilities, quality of life and frequency of depression for our strong cohort of patients with PACNS in the longest reported follow-up in the literature to date and the first evaluation of the quality of life and incidence of depression in these patients. Of 78 patients, 27 responded to the questionnaires (34.6 percent). Mean follow-up was 5.5 years (± 4.7). Seventy percent had mild disability, and 5 percent had severe disability. Around half of the patients had no mobility problem and no problems with usual activities, and two-thirds had no problems with self-care. Physician assessment with the Modified Rankin Scale showed that the majority of PACNS patients had mild long-term disability with a median disability score of one. Approximately 70 percent of patients had minimal or no depression. Mortality was 11 percent.
Advertisement
As our experience with and knowledge of PACNS and RCVS has grown, rheumatologists and neurologists alike grow closer toward demystifying these mimics and providing precise diagnoses for affected patients. Much work remains to be done to assess the pathogenesis and etiologies of both conditions. At the RJ Fasenmyer Center for Clinical Immunology’s CNS Vasculopathy Program, we are currently looking for biomarkers in CSF to better elucidate these mechanisms.
Dr. Hajj-Ali is Associate Director of the Center for Vasculitis Care and Research in the Department of Rheumatic and Immunologic Diseases. Dr. Calabrese is Director of the R.J. Fasenmyer Center for Clinical Immunology.
Advertisement
Advertisement

Routine capture of standardized neuroperformance data may expand and refine investigations

Nearly one-fifth of such cases fulfill 2024 McDonald criteria based on biomarkers

Adequate dosing may improve outcomes in well-selected patients, large Cleveland Clinic series suggests

Reimagining the outpatient neurological visit with routine capture of neuroperformance data

Free portal helps researchers classify and share data using the IC-CoDE framework

Large study shows rural patients are less apt to be discharged to inpatient rehab, hampering outcomes

Updates on this fast-evolving therapeutic landscape from a leading trialist

Advanced surgical suite in our soon-to-open facility promises to redefine care standards