Locations:

Why and how Cleveland Clinic achieves repair in 99% of patients
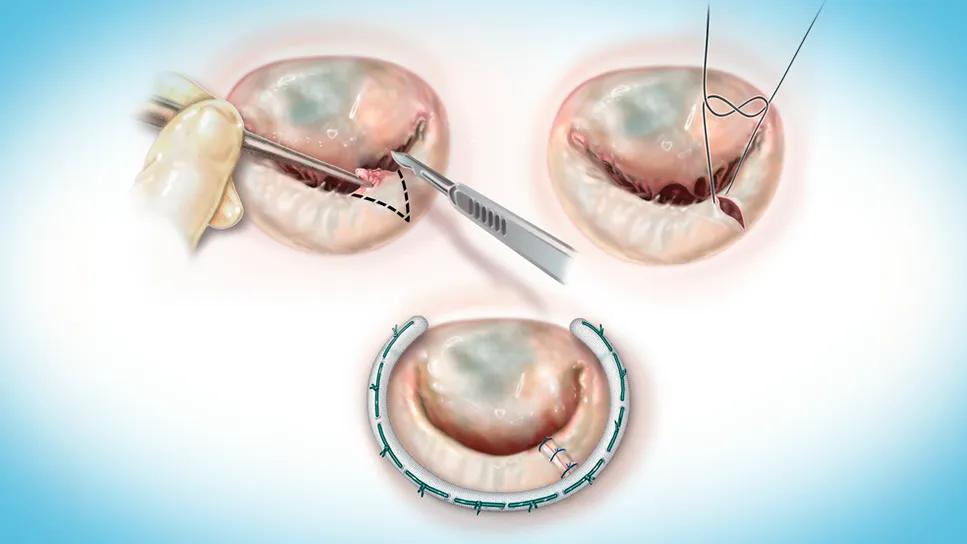
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a8e845a0-0ea9-46e3-a00a-1221d2c9ea43/triangular-resection-feature)
three-panel illustration of a mitral valve operation
When cardiovascular providers refer a patient with severe mitral valve prolapse for surgery, they are wise to prioritize a center’s likelihood of performing mitral valve repair over mitral valve replacement, according to Marc Gillinov, MD, Chair of Thoracic and Cardiovascular Surgery at Cleveland Clinic.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“When repair is feasible, it is the best option for degenerative mitral valve disease,” says Dr. Gillinov, citing superior long-term survival. “Repair of the prolapsing valve restores a patient’s normal life expectancy, whereas replacement does not.” Moreover, repair avoids the lifelong anticoagulation required with replacement using a mechanical valve and offers greater durability than replacement with a bioprosthetic valve.
Dr. Gillinov notes that Cleveland Clinic is able to treat 99% of its patients with degenerative mitral valve disease using repair rather than replacement — a considerably higher share than national rates of 90% or lower. He attributes that near-universal repair rate to Cleveland Clinic’s large volume of mitral valve cases and team of mitral valve surgeons who specialize in those cases day in and day out.
“We often operate with two highly experienced mitral valve surgeons together, at least for certain parts of the repair, particularly in complex cases,” says Tarek Malas, MD, one of that team of cardiothoracic surgeons specializing in mitral valve disease. “This contributes to our ability to successfully offer repair so often.”
Drs. Malas and Gillinov also attribute their team’s high repair rate to Cleveland Clinic’s algorithm for mitral valve repair, which is built around five techniques accessible to virtually all cardiac surgeons — (1) triangular resection (Figure), (2) sliding repair, (3) creation of artificial chordae, (4) commissuroplasty and (5) annuloplasty.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2fe80346-e2c8-403e-bdfa-1f529710baea/triangular-resection-inset)
Figure. Three key steps of a triangular resection, one of the five cornerstone techniques of mitral valve repair championed by Cleveland Clinic. When combined with an annuloplasty (panel C), triangular resection is all that’s needed to repair segmental posterior leaflet prolapse, one of the most common lesions in degenerative mitral valve disease.
This organized approach to the valve, together with Cleveland Clinic’s experience from over 1,000 mitral valve operations each year, is likewise instrumental to the program’s exceptionally low operative mortality for isolated mitral valve repair, which has been less than one death per 1,000 cases for more than a decade. “I tell my patients this is as safe as gallbladder surgery,” Dr. Gillinov says.
Despite these successes and the near-universal repair rate, Cleveland Clinic surgeons offer expert mitral valve replacement when required, such as in the setting of rheumatic heart disease or when the mitral valve is so calcified or compromised by endocarditis that repair is not feasible. Another instance is advanced age, although repair can be safe for many older patients. “We regularly offer repair to patients in their mid-70s, and it may be the safest, quickest operation even for some 80-year-olds with mitral valve prolapse,” Dr. Gillinov says.
The average age at surgery for mitral valve prolapse is 59 years, which puts a premium on the durability of mitral valve repair. In the contemporary era, a large majority of patients do not require reintervention for up to 20 years after repair, although about 10% develop recurrent mitral regurgitation (MR) at 10 years. “For this reason, every patient should get an echocardiogram once a year after a successful repair,” Dr. Gillinov notes.
To ensure repair durability, the Cleveland Clinic team is meticulous about minimizing residual MR in the operating room, which means ensuring a grade of zero or close to zero. “Residual MR after surgery can compromise length of survival and repair durability, and it raises the risk of heart failure down the line,” Dr. Malas says. “So we always try to achieve an MR grade below 1+. We won’t leave the operating room with MR above that. We work with our expert echocardiographers to find the source of any regurgitation and revise the repair as needed. In very rare cases, we will replace the valve if necessary to give the patient the best possible result.”
Advertisement
This vigilance is borne out by recent data. In a newly published retrospective study of 563 patients undergoing mitral valve repair at Cleveland Clinic via robotic assistance or sternotomy from 2020 to early 2024 (JTCVS Open. 2025 Epub 10 Nov), 98% of patients had no MR on their transthoracic echocardiogram before discharge.
In those cases when a mitral valve repair fails over time, many centers tend to favor valve replacement over re-repair, but not Cleveland Clinic.
“Currently, we can perform re-repair in 70% to 80% of patients who have failure of a previous repair,” Dr. Gillinov says. “We have the experience to understand when re-repair is and is not appropriate. We perform re-repairs almost every week, and that frequency is important because re-repair requires specialized expertise on the surgical side and on the echocardiographic side, to determine what’s wrong with the valve.”
This approach was bolstered by findings from a retrospective study of Cleveland Clinic reoperations after early and late failure of mitral valve repair among 330 patients from 2008 to 2020 (J Thorac Cardiovasc Surg. 2024;167[4]:1251-1262.e8), with 28% of patients undergoing re-repair and 72% undergoing valve replacement. Re-repair was associated with zero hospital deaths and with long-term survival that was higher than with replacement and comparable to that of the age- and sex-matched general U.S. population. At seven years after reoperation, freedom from severe MR was 93% in the re-repair group and freedom from reoperation was 86%.
Advertisement
“Over the last five years of the study, we saw a trend toward more aggressive use of re-repair,” Dr. Gillinov notes. “More than 90% of those re-repairs were done for annuloplasty dehiscence, systolic anterior motion and adverse ventricular remodeling. Replacement was still performed for patients with progressive fibrosis or mitral stenosis.”
“If we think we can perform a good repair based on the valve anatomy, we will re-repair,” Dr. Malas adds. “But often these are cases with limited tissue, so we ultimately decide between re-repair and replacement when we actually examine the valve directly in the operating room.”
Beyond the likelihood of repair whenever feasible, Drs. Gillinov and Malas identify other leading considerations when referring patients for treatment of mitral valve prolapse:
Advertisement
“We’re especially vigilant about offering concomitant surgical ablation of atrial fibrillation to all appropriate patients undergoing mitral valve repair,” Dr. Malas says. “It’s beneficial for getting patients out of atrial fibrillation as well as for prolonging survival. It’s also a class I guideline indication, yet national rates of concomitant ablation for atrial fibrillation are very low.”
A final essential piece of advice is to refer early — at first recognition of severe MR, even if symptoms aren’t yet present. “When physicians wait to refer until the patient starts to develop atrial fibrillation or heart failure or left ventricular dysfunction, cardiac damage has already occurred and the chance of a normal life expectancy after successful repair declines,” Dr. Gillinov observes. “Yet more than half of patients are referred late. There is no advantage to waiting to fix severe MR, but the potential downside is clear.”
Advertisement

NIH-funded comparative trial will complete enrollment soon

Safety and efficacy are comparable to open repair across 2,600+ cases at Cleveland Clinic

Two surgeons share insights on weighing considerations across the lifespan

An overview of growth in robot-assisted surgery, impressive re-repair success rates and more

Judicious application yields a 99.7% repair rate and 0.04% mortality
Cleveland Clinic series supports re-repair as a favored option regardless of failure timing

A call for surgical guidelines to adopt sex-specific thresholds of LV size and function
Cleveland Clinic series shows re-repair is feasible with excellent midterm results