Locations:

Cleveland Clinic series shows re-repair is feasible with excellent midterm results
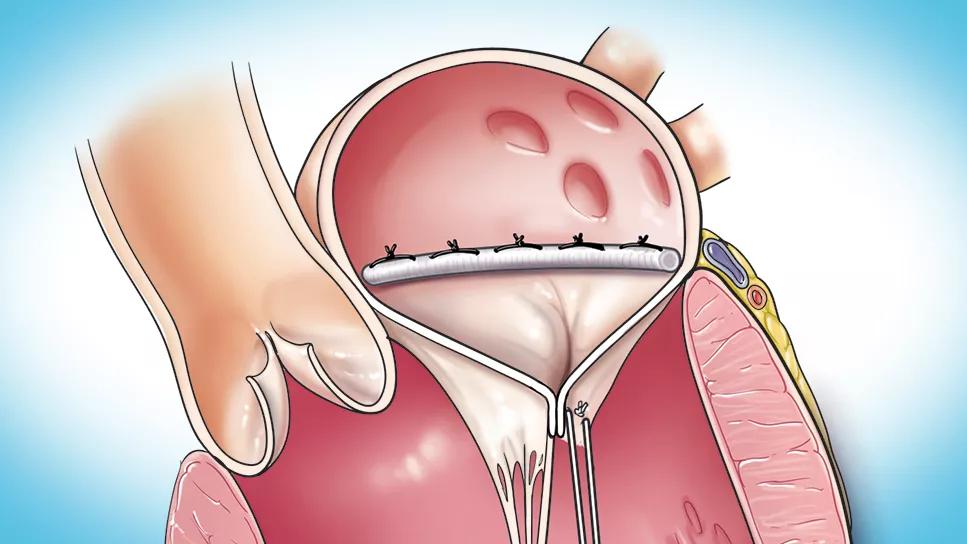
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9bab83b5-6572-4ad5-b861-875623103d42/completed-mitral-valve-repair-1)
illustrations of chambers of the human heart
An uncommon failure of initially successful mitral valve (MV) posterior leaflet repair with creation of artificial chordae involves the development of posterior leaflet prolapse and apparent elongation of the chordae, caused by normalization of left ventricular morphology. In such cases, re-repair is likely to be safe, effective and durable whether it’s accomplished with creation of new, shorter artificial chordae or with posterior leaflet resection (with or without placement of a new annuloplasty). So found a Cleveland Clinic series of 10 patients who underwent MV re-repair for this unusual complication, as recently described in JTCVS Techniques (Epub 21 Oct 2023).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“In a patient who had posterior leaflet repair and then develops recurrent mitral regurgitation with pseudo-elongation of the artificial chordae because of left ventricular reverse remodeling, the problem can often be fixed in a straightforward manner with re-repair of the mitral valve,” says the study’s senior author, A. Marc Gillinov, MD, Chair of Thoracic and Cardiovascular Surgery at Cleveland Clinic. “When anatomically possible, we prefer this approach to valve replacement.”
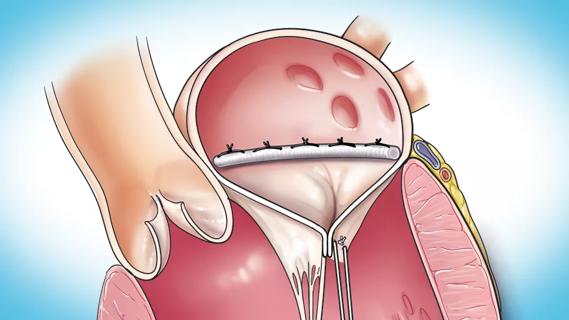
Mitral regurgitation due to degenerative posterior leaflet prolapse can be addressed by two equally effective repair strategies: leaflet resection or creation of artificial chordae. In rare cases, the latter approach leads to failure as the left ventricle undergoes reverse remodeling, causing prolapse of the posterior leaflet and pseudo-elongation of artificial chordae (Figure).
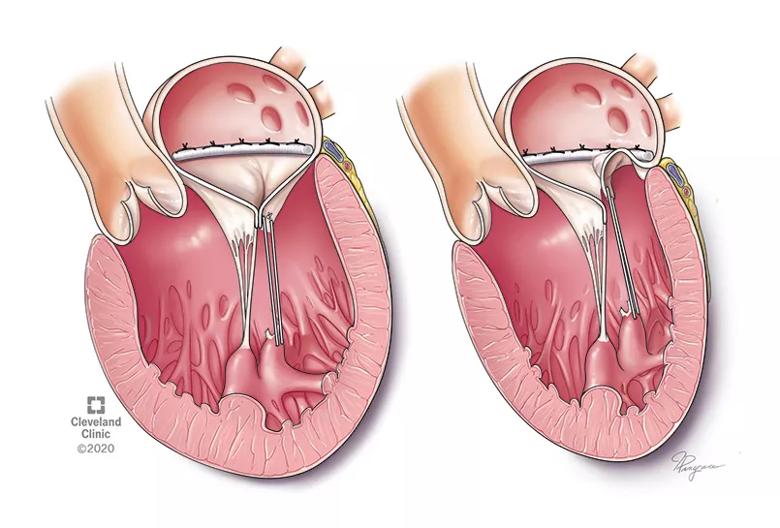
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3e5091e9-89fa-46ad-9bf3-db224ae5b492/23-HVI-4394262-CQD-Inset1_jpg)
Figure. Recurrent mitral regurgitation due to chordal pseudo-elongation. Left: A seemingly perfect mitral valve repair using artificial chordae in a markedly enlarged left ventricle. Right: As the ventricle shrinks, the artificial chordae appear too long (chordal pseudo-elongation) for the remodeled left ventricle, leading to recurrent posterior leaflet prolapse. Reprinted from Bernabei et al., JTCVS Techniques (S2666-2507[23]00397-8), ©2023, with permission from Elsevier.
In two recent articles, Cleveland Clinic cardiothoracic surgeons discuss the techniques of MV re-repair and its advantages over valve replacement (Oper Tech Thorac Cardiovasc Surg. 2021:26[1]:42-65, and J Thorac Cardiovasc Surg. 2022:S0022-5223[22]01023-6).
Advertisement
Their current study was designed to assess outcomes of MV re-repair specifically for repair failure accompanied by posterior leaflet prolapse with pseudo-elongation of the artificial chordae.
During a recent 15-year period, 11 patients presented to Cleveland Clinic with moderately severe or severe mitral regurgitation due to recurrent prolapse following initial successful posterior leaflet repair with artificial chordae and annuloplasty. Of the 11 patients, six were male, mean age was 58 years, median time between initial operation and reoperation was 14 months, and left ventricular diameters were reduced across the cohort.
Reoperation consisted of valve replacement in one patient, with the other 10 undergoing re-repair: half had creation of new, shorter artificial chordae and half had posterior leaflet resection. Eight patients had placement of a new annuloplasty.
No operative mortality or major complications occurred among the 11 patients. Last echocardiographic follow-up (at a median of 20 months) found no more than mild mitral regurgitation.
The series demonstrated that re-repair for failure of initial MV repair in this setting of posterior leaflet prolapse due to ventricular remodeling is feasible and effective with excellent midterm outcomes. Re-repair was equally durable whether accomplished with leaflet resection or placement of shorter artificial chordae.
The study authors note that careful selection of the initial repair technique can help avoid development of recurrent mitral regurgitation due to posterior leaflet prolapse as ventricular morphology normalizes.
Advertisement
“In general, in patients with an enlarged left ventricle, one must be mindful of potential remodeling and, if placing artificial chords, make the appropriate length adjustments to avoid recurrent leaflet prolapse if reverse remodeling ensues,” advises Cleveland Clinic cardiothoracic surgeon Tarek Malas, MD.
Advertisement
Advertisement

NIH-funded comparative trial will complete enrollment soon

Safety and efficacy are comparable to open repair across 2,600+ cases at Cleveland Clinic

Why and how Cleveland Clinic achieves repair in 99% of patients

Two surgeons share insights on weighing considerations across the lifespan

An overview of growth in robot-assisted surgery, impressive re-repair success rates and more

Judicious application yields a 99.7% repair rate and 0.04% mortality
Cleveland Clinic series supports re-repair as a favored option regardless of failure timing

A call for surgical guidelines to adopt sex-specific thresholds of LV size and function