Locations:

Practice pointers for managing diabetic kidney disease

By Jonathan J. Taliercio, DO; George Thomas, MD; Georges N. Nakhoul, MD, Med; Tushar J. Vachharajani, MD and Ali Mehdi, MD, MEd
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Diabetic kidney disease is a major cause of chronic kidney disease and the most common cause of end-stage kidney disease. Before the sodium-glucose cotransporter-2 (SGLT-2) inhibitors were introduced, the nephrology community had not had much to celebrate in the management of diabetic kidney disease since the landmark trials of renin-angiotensin system blockers 20 years ago.1–3 Since that time, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers have been the cornerstone of managing proteinuric diabetic and nondiabetic kidney disease. Fast-forward 20 years, and SGLT-2 inhibitors have emerged as a major addition to our toolkit in the management of diabetic kidney disease.
Tsushima et al4discuss the role of SGLT-2 inhibitors in managing patients with type 2 diabetes and highlight the updated 2020 treatment guidelines from the American Diabetes Association and the American Association of Clinical Endocrinologists.5,6 The authors thoroughly highlight the overwhelmingly beneficial cardiovascular, kidney, and metabolic effects of this new class of medications that is taking many different medical specialties by storm.
Here, we would like to expand the discussion on the kidney effects of the SGLT-2 inhibitors. We will highlight only the SGLT-2 inhibitors that have data on primary and secondary renal outcomes; however, we suspect that the benefits are a class effect. We also summarize the 2020 KDIGO (Kidney Disease: Improving Global Outcomes) guidelines, which emphasize early and extended use of SGLT-2 inhibitors in patients with diabetic kidney disease.7
Advertisement
As reviewed by Tsushima et al, 4 large randomized controlled trials proved SGLT-2 inhibitors to be beneficial in patients with type 2 diabetes in terms of primary cardiovascular outcomes and secondary renal endpoints (Table 1).8–14 These results paved the way for the CREDENCE trial12 (Canagliflozin and Renal Events in Diabetes With Established Nephropathy Clinical Evaluation), which was the first major randomized, placebo-controlled multicenter study to evaluate primary renal composite endpoints consisting of end-stage kidney disease, a doubling of serum creatinine level, or death from a renal or cardiovascular cause.
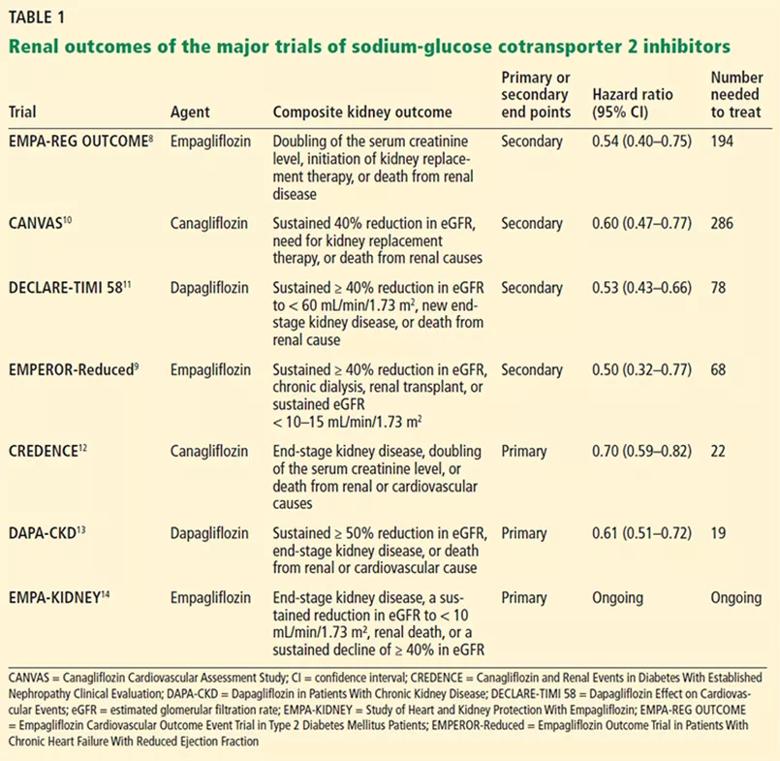
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ef4753cf-5fc5-41a5-a8ba-254bf865819d/21-URL-2135108-CQD_jpg)
The results were overwhelmingly positive, with a 30% relative risk reduction (hazard ratio [HR] 0.70, 95% confidence interval [CI] 059–0.82, P = .00001) with canagliflozin compared with placebo. This astonishing outcome was in patients who were already taking maximally tolerated doses of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. To accentuate the point, the landmark trials of renin-angiotensin system inhibitors such as the Irbesartan Diabetic Nephropathy Trial2 and the Reduction of Endpoints in NIDDM With the Angiotensin II Antagonist Losartan study3 demonstrated a 33% and 25% reduction in doubling in serum creatinine, respectively, while canagliflozin had a 40% reduction.
Even more intriguing is the newly published DAPA-CKD (Dapagliflozin in Patients With Chronic Kidney Disease) trial, which has confirmed the renal benefits of CREDENCE, and has expanded the population eligible for treatment with an SGLT-2 inhibitor.13
Advertisement
The DAPA-CKD trial13 was a large, multicenter, randomized controlled trial that enrolled 4,304 participants to receive dapagliflozin (10 mg once daily) or placebo. In contrast to the CREDENCE trial, which included only patients with type 2 diabetic proteinuria (with albumin-to-creatinine ratios of 300–5,000 mg/g) with an estimated glomerular filtration rate (eGFR) between 30 and 90 mL/min/1.73 m2, the DAPA-CKD trial enrolled patients with chronic kidney disease with lower eGFRs (between 25 and 75 mL/min/1.73 m2), less proteinuria (albumin-to-creatinine ratios of 200–5,000 mg/g), with or without type 2 diabetes. Approximately two-thirds of participants enrolled had type 2 diabetes, and 98% of all participants were on a stable dose of an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker.
The primary composite outcome was a sustained decline in eGFR of at least 50%, end-stage kidney disease, or death from kidney or cardiovascular causes.
The independent data monitoring committee stopped the trial after a median of 2.4 years, after primary efficacy end points were achieved. There was a 39% reduction in the primary composite outcome in the dapagliflozin group (HR 0.61, 95% CI 0.51–0.72, P < .001), and the number needed to treat was 19 (95% CI 15–27). Results were similar regardless of diabetes status, and the beneficial kidney outcomes were independent of glycemic control. Dapagliflozin also achieved a 31% risk reduction in all-cause mortality (HR 0.69, 95% CI 0.53–0.88, P = .004) and a 44% risk reduction in worsening renal function or death from kidney failure (HR 0.56, 95% CI 0.45–0.68, P < .0001). Interestingly, the incidence of serious adverse events in the dapagliflozin group was similar to that in the placebo group (33.9% vs 29.5%), with ketoacidosis not reported in the dapagliflozin group and severe hypoglycemia not observed in the nondiabetic population.
Advertisement
Given the emerging data, Kidney Disease: Improving Global Outcomes (KDIGO) recently published their inaugural 2020 practice guidelines for diabetes management in chronic kidney disease patients.7 KDIGO goes beyond what the American Diabetes Association and American Association of Clinical Endocrinologists guidelines say, recommending SGLT-2 inhibitors and metformin as first-line drugs for diabetic kidney disease. We summarize here the key points as they pertain to antihyperglycemic therapies in patients with diabetes and chronic kidney disease.
Glycemic control for management of patients with type 2 diabetes and chronic kidney disease should include lifestyle therapy; first-line drug treatment includes metformin and an SGLT-2 inhibitor, and additional drug therapies as needed for glycemic control. Specifically:
Metformin is a preferred first-line agent due to its glucose-lowering control, tolerability, and low cost. SGLT-2 inhibitors are relatively weak antiglycemic drugs with smaller reductions of hemoglobin A1c. The recommendation to add SGLT-2 inhibiters in combination with metformin is primarily for the beneficial effects of slowing the progression of nephrologic and cardiovascular disease and not for hemoglobin A1c control.
Advertisement
Hemoglobin A1c targets are individualized, ranging from less than 6.5% to less than 8.0% in patients with diabetes and chronic kidney disease not treated with dialysis (grade 1C recommendation: recommended, but low-quality evidence).
We believe that frontline clinicians should initiate SGLT-2 inhibitors for patients with type 2 diabetes and diabetic kidney disease who have an eGFR of at least 30 mL/min/1.73 m2. Maximal treatment with an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker is highly recommended before starting the SGLT-2 inhibitor but is not an absolute requirement in patients who cannot tolerate renin-angiotensin system blockade.
Deferring initiation of SGLT-2 inhibitors to a specialist (a nephrologist or endocrinologist) will result in a faster progression of diabetic kidney disease irrespective of glycemic control, and it is crucial to initiate these medications as early as possible. SGLT-2 inhibitors are contraindicated if the eGFR is less than 25 mL/min/1.73 m2 (see below), and later initiation even with acceptable but lower eGFR ranges may be more problematic as it relates to the expected acute drop in eGFR.
Efficacious doses of SGLT-2 inhibitors that have been studied in diabetic kidney disease are canagliflozin 100 mg, empagliflozin 10 mg, or dapagliflozin 10 mg.
Prescribers should be aware of the initial reversible drop in eGFR of approximately 5 to 8 mL/min/1.73 m2 (up to a 20% drop) in the first 2 weeks after starting SGLT-2 inhibitors, which is due to the hemodynamic effects of the drug. This decrease is analogous to the hemodynamic effects of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. This mild reduction in eGFR does not require discontinuation of the drug.
We anticipate the lower limit of kidney function below which SGLT-2 inhibitors cannot be started will continue to be challenged. Currently, canagliflozin and empagliflozin initiation is contraindicated if the eGFR is less than 30 mL/min/1.73 m2, while dapagliflozin lowered the eGFR threshold to less than 25 mL/minute/1.73 m2 as a result of the DAPA-CKD trial.13 The Study of Heart and Kidney Protection With Empagliflozin (EMPA-KIDNEY)14 is recruiting patients whose eGFR can be as low as 20 mL/min/1.73 m2.
Educate the patient about the “sick day rule.” SGLT-2 inhibitors should be held in periods of illness accompanied by decreased oral intake or increased volume losses. Hypovolemia and altered arteriolar hemodynamics may predispose patients to ischemic tubular kidney injury.
The risks and benefits of therapy should be assessed in patients with a history of urinary tract infections, genitourinary yeast infections, or diabetic ketoacidosis.
The scope of the KDIGO guidelines was limited to diabetic kidney disease, and the work group did not incorporate recommendations for patients who have chronic kidney disease but no diabetes. All of the aforementioned studies exclusively studied proteinuric diabetic kidney disease, with the exception of the DAPA-CKD trial, in which only one-third (n = 1,398) of the participants did not have diabetes, and which still demonstrated kidney benefits in this subgroup.
In subgroup analysis of the DAPA-CKD trial, 50% of nondiabetic kidney disease patients (HR 0.50; 95% CI 0.35–0.72) vs 36% of diabetic kidney disease patients (HR 0.64, 95% CI 0.52–0.79) met the primary composite outcome (sustained decline in eGFR of at least 50%, end-stage kidney disease, or death from kidney or cardiovascular causes). Neither diabetic ketoacidosis nor severe hypoglycemia was observed in participants without type 2 diabetes.
Questions remain about whether SGLT-2 inhibitors have kidney benefits in patients with diabetes who have chronic kidney disease without proteinuria, or in patients without diabetes who have chronic kidney disease without proteinuria.
EMPA-KIDNEY14 will hopefully shed more light on this population. The study is actively enrolling 6,000 patients who have chronic kidney disease with or without type 2 diabetes with eGFRs of 20 to less than 45 mL/min/1.73 m2, and eGFRs of 45 to less than 90 mL/min/1.73 m2 with less albuminuria (albumin-creatinine ratios ≥ 200 mg/g). The primary composite outcome includes several hard kidney disease outcomes. The EMPA-KIDNEY results are expected in the summer of 2022.
Another important patient population that has been excluded from these trials is kidney transplant recipients. Type 2 diabetes was listed as the cause of their end-stage kidney disease in 31% of patients who received kidney transplants in 2019.15 These patients may benefit from SGLT-2 inhibitors, but concerns include the risk of genitourinary infections and the uncertainty and additional testing that may be required to differentiate acute rejection from the expected rise in serum creatinine at time of initiation. We hope to get more information about this subgroup in the future.
SGLT-2 inhibitors have blown the doors wide open in the management of diabetic kidney disease. Further, additional classes of medications appear to be on the horizon. A novel nonsteroidal mineralocorticoid receptor antagonist (finerenone),16 an endothelin receptor antagonist (atrasentan),17 and glucagon-like peptide 1 receptor agonists are some promising agents for slowing the progression of diabetic kidney disease. The long-awaited future of multitargeted treatment for diabetic kidney disease is finally here!
Editor’s note: This article originally appeared in the Cleveland Clinic Journal of Medicine.
Disclosures
Jonathan J. Taliercio, DO, is an EMPA-KIDNEY and SONAR co-investigator. Georges N. Nakhoul MD, MEd, is an EMPA-KIDNEY co-investigator. George Thomas, MD, is an EMPA-KIDNEY principal investigator. All other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
References
Advertisement

Pediatric urologists lead quality improvement initiative, author systemwide guideline

Fixed-dose single-pill combinations and future therapies

Reproductive urologists publish a contemporary review to guide practice

Two recent cases show favorable pain and cosmesis outcomes

Meta-analysis assesses outcomes in adolescent age vs. mid-adulthood

Proteinuria reduction remains the most important treatment target.

IgA nephropathy is a relatively common autoimmune glomerular disease that can be diagnosed only by biopsy

Oncologic and functional outcomes are promising, but selection is key