Locations:

Concomitant AF ablation and LAA occlusion strongly endorsed during elective heart surgery
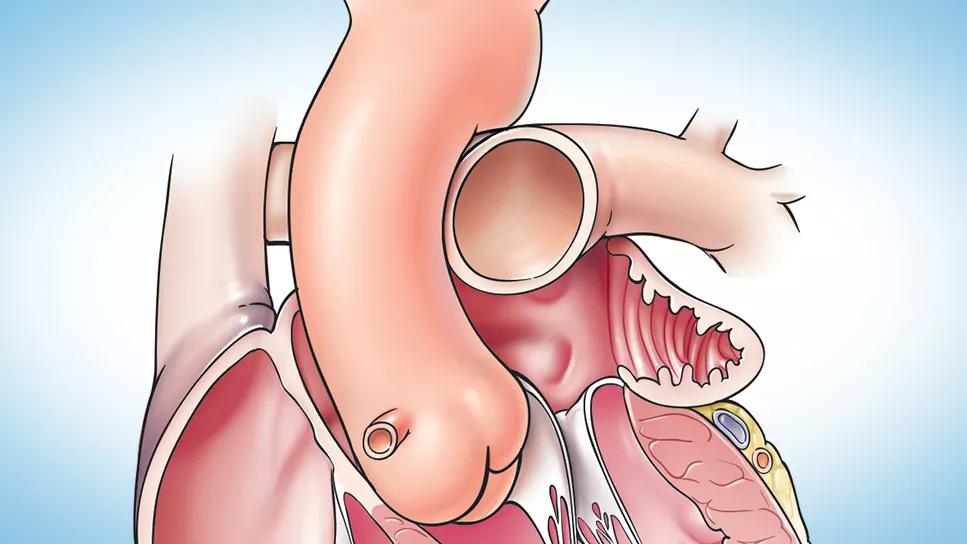
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7584f9a4-7330-40e4-a22d-0041f25a3408/heart-left-atrial-appendage)
illustration of the human heart focused on the left atrial appendage
Nonemergency cardiac operations in patients with atrial fibrillation (AF) should include surgical left atrial appendage (LAA) occlusion during the operation, according to new 2023 practice guidelines on the surgical treatment of AF from the Society of Thoracic Surgeons (STS). The guidelines, published in the Annals of Thoracic Surgery (Epub 27 Jan 2024), also reinforce the long-term benefits of surgical ablation of AF during nonemergency cardiac operations.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“It’s important that every single person with atrial fibrillation undergoing elective open-heart surgery have their atrial fibrillation treated and their left atrial appendage managed,” says A. Marc Gillinov, MD, Chair of Thoracic and Cardiovascular Surgery at Cleveland Clinic and one of eight members of the writing committee that produced the guidelines. He sees the recommendations as a wake-up call to the surgical community. “Currently, only a small percentage of patients with atrial fibrillation undergo treatment during a concomitant procedure,” he notes. “It’s viewed as less important. However, it’s important for patients, because it lowers their risk of stroke and improves longevity.”
The 2023 guidelines are an update to 2017 STS guidelines on the subject. The update was undertaken to reflect considerable evidence, some from randomized clinical trials, that emerged since the prior version was issued.
Both the 2017 and 2023 guidelines give a highest-level (class I-A) recommendation to surgical ablation for patients with AF undergoing a first-time nonemergency operation on the mitral valve, citing safety and long-term benefits. Whereas the 2017 guidelines gave a I-B recommendation to surgical ablation for AF during concomitant aortic valve and coronary artery bypass operations, the 2023 guidelines extend this I-B endorsement to all first-time nonemergency heart surgeries.
In the 2017 guidelines, LAA excision or exclusion in conjunction with surgical ablation of AF was deemed “reasonable” and given a class IIa-C recommendation. The 2023 update has upgraded this to a class I-A endorsement.
Advertisement
“Recent data confirm that in cardiac surgery patients with atrial fibrillation, treating the LAA is beneficial in reducing morbidity from thromboembolic complications,” Dr. Gillinov explains. “It is recommended for all patients undergoing first-time nonemergent cardiac surgery, whether or not surgical ablation is performed concomitantly.”
The 2023 guidelines add a class IIb-B recommendation for consideration of isolated surgical LAA obliteration in patients with long-standing persistent AF at high stroke risk in whom long-term oral anticoagulation is contraindicated or has failed.
Data on the value of excluding the LAA from the circulation is encouraging enough that some researchers are exploring whether the LAA should be treated during surgery in selected patients who have never been diagnosed with AF. A large, multicenter, industry-sponsored clinical trial addressing this issue is underway and expected to be completed in 2032. “This prophylactic treatment may or may not be a good idea,” Dr. Gillinov says.
The 2023 guidelines addressed, for the first time, treatment for patients with symptomatic valve disease and AF at low to intermediate surgical risk. The writing committee gave a level IIa-B recommendation to surgical valve repair or replacement with concomitant surgical ablation and LAA occlusion, rather than transcatheter valve repair or replacement alone, for restoring sinus rhythm and improving long-term outcomes.
For all patients with AF, the new guidelines reiterate the value of multidisciplinary heart team assessment, treatment planning and follow-up rhythm assessment for optimizing patient outcomes.
Advertisement
“This guideline update is welcome,” notes Oussama Wazni, MD, MBA, Section Head of Cardiac Electrophysiology and Pacing at Cleveland Clinic. “Electrophysiologists here and elsewhere value the surgical management of atrial fibrillation. For patients with atrial fibrillation undergoing heart surgery, it is highly important to address their atrial fibrillation at the time of surgery whenever that is possible.”
Advertisement
Advertisement

AVANT GUARD trial extends first-line role for ablation beyond paroxysmal atrial fibrillation

LAA closure may be compelling option in atrial fibrillation ablation patients at high risk of both stroke and bleeding

UK experts compare and contrast the latest recommendations

While results were negative for metformin, lifestyle counseling showed surprising promise

Investigational pulsed-field ablation system also yielded procedural efficiencies

ACC/AHA panel also upgrades catheter ablation recommendations
For the first time, risk is shown after accounting for underlying contributions of pulmonary disease

Retrospective analysis finds “hypoxic and sleepy” subtype to confer greatest risk