Locations:

Surgeons use the single-port robot to achieve transvesical access to the vagina
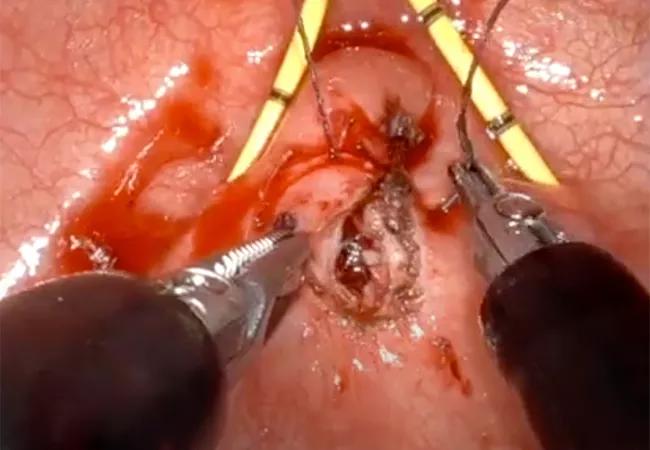
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/86d6e7f3-f923-46d9-b472-f4e77b582511/22-URL-2928717-650x450-1_jpg)
22-URL-2928717 650×450
Cleveland Clinic urologists have reported good outcomes in recent cases that have utilized the single-port (SP) robotic system to gain transvesical access for vesicovaginal fistula (VVF) repair. While vaginal or abdominal access is the mainstay for VVF repair, in select cases the transvesical approach, which means directly through the bladder, is a possible alternative.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In many patients, closing the fistula through the vaginal route is successful. However, some patients with complex or recurrent fistulae may be better suited for an abdominal approach, which may include open, laparoscopic or robot-assisted surgery, all of which can utilize the omentum flap to close the fistula hole and create a barrier between the bladder and vagina to reduce the risk of recurrent malformation.
In a recent case, female pelvic medicine and reconstructive surgeon Sandip Vasavada, MD, was faced with a challenge. The patient had a complicated abdomen and no omentum flap as a result of previous abdominal surgeries. Proceeding with limited flap options could have led to an increased likelihood of postoperative morbidity.
Vaginal access was also not an option because of clinical indications and patient preference. The team and the patient decided to proceed using the single-port robot with the transvesical approach to access the VVF.
Dr. Vasavada, who collaborated with Mohamed Eltemamy, MD, a staff member in the section of Urology/Advanced Urological Robotic & Laparoscopy on this case, says this approach is rarely warranted for VVF repair. But given the patient-specific challenges, it was an ideal choice.
In the intraoperative video below, the surgeons separate the hole or “the communication between the bladder and the vagina.” Then they raise the flap tissue around it and close it sequentially side-by-side.
Video content: This video is available to watch online.
View video online (https://www.youtube.com/embed/xJVFPxXW3qM?feature=oembed)
Single-Port Robot-Assisted Transvesical Repair of a Vesicovaginal Fistula (Graphic)
“The patient had no complications and was discharged the same day. It’s not going to be like this case every time, but it’s appropriate to consider this approach in extreme circumstances like hers.”
Advertisement
Results were similar in a different case with a patient who had a complicated abdomen and had previously failed two vaginal surgeries. “It was a difficult situation, and success rates decline after each attempt; but, we decided if we can access it from inside the bladder, we will. And that’s where the utility of the single-port robotic approach really comes into play,” Dr. Vasavada notes.
While indications are still evolving, patients with complicated abdomens, limited interposing flap options, an otherwise satisfactory bladder capacity, and no need for radiation after surgery may be candidates for this approach.
Advertisement
Advertisement

New moniker brings clarity to this complex condition

A device implanted at the ankle joins the lineup of third-line treatments

Aiming for earlier detection of endometrial cancer in an era of increasing incidence

Minimally invasive surgery is the preferred approach in many cases, but not all

Patients deserve timely diagnosis and a multidisciplinary approach

Data point to potential for targeted preconception planning

Reproductive psychiatry helps patients balance medication-related risks

Molecular profiles help guide referral and care planning