Locations:

Academia, industry and government leaders develop consensus priorities
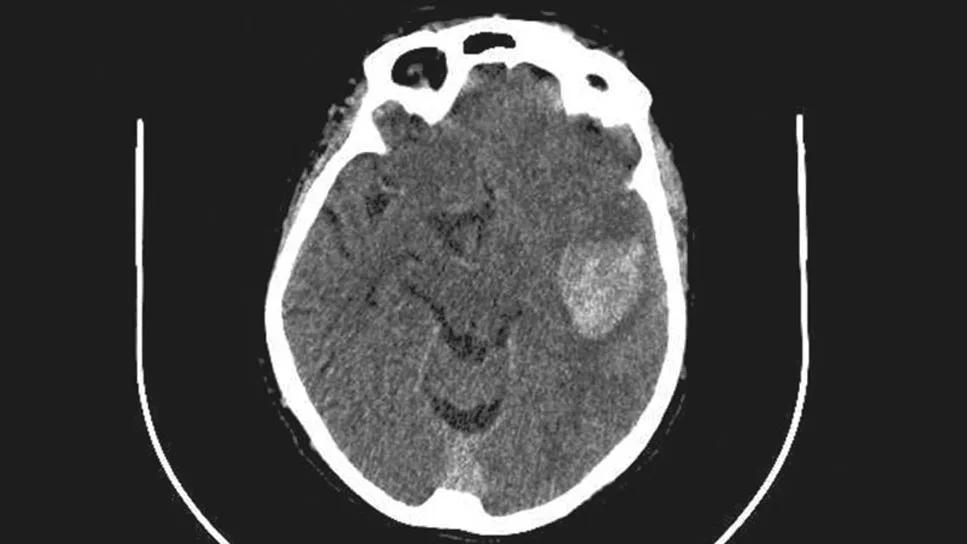
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e219d9da-09fa-4c6d-99ac-7dedd945497f/intracerebral-hemorrhage-imaging-study)
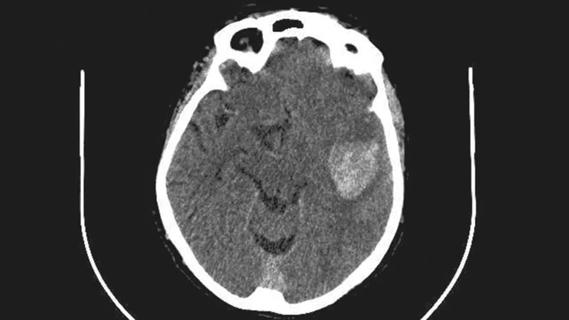
brain scan with white lesion on right side
Future research efforts into intracranial hemorrhage (ICH) management should focus on the impact of early intervention, minimally invasive evacuation, new surgical technology and the role of artificial intelligence (AI). These and other recommendations were put forth by the ARISE II (Roundtable Discussion with Industry and Stroke Experts) Consortium, consisting of multidisciplinary clinical experts, healthcare industry leaders, and FDA and NIH representatives. Their consensus recommendations were recently published online ahead of print by the Journal of NeuroInterventional Surgery.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“The ARISE process is different from that of developing management guidelines from professional medical societies based on the clinical literature,” says lead and corresponding author Mark Bain, MD, MS, a vascular neurosurgeon at Cleveland Clinic. “Instead, these recommendations arose from a broad and varied group of interested parties in the same room discussing what is needed in the field, what is technically feasible and what is likely to be funded.”
Sponsored solely by participating private sector companies, the ARISE group receives no government funding. They have published previous consensus statements on managing chronic subdural hematomas (Stroke. 2024;55[5]:1438-1448) and approaches to improved brain arteriovenous malformation management (Stroke. 2024;55[5]:1449-1463).
The current consensus recommendations on ICH management cover a wide range of topics, from prehospital triage to post-ICH rehabilitation, with critical issues identified and recommendations for future efforts to address unanswered questions. Key takeaways are recapped below.
Evidence is strong that timely intervention for ICH is critical, particularly to promptly and aggressively lower systolic blood pressure to 130 to 150 mmHg, reverse anticoagulants, and transfer patients to minimally invasive surgical evacuation centers. Although mobile stroke units with a portable CT scanner can quickly identify ICH and provide critical interventions, they are prohibitively expensive for many communities and pose logistic challenges integrating into existing emergency medical services. Research is needed on additional optimal ways to get patients the help they need quickly and safely.
Advertisement
A number of medications have undergone preliminary research for ameliorating secondary brain injury from ICH. They include:
Further studies are needed to assess these medications’ clinical effectiveness.
“Open craniotomy hematoma evacuation has not demonstrated benefit in large clinical trials,” Dr. Bain says. “Whether minimally invasive strategies such as stereotactic catheter drainage, thrombolysis and endoscopic procedures could provide benefit from hematoma evacuation is being actively explored.”
Cleveland Clinic participated in the ENRICH trial, which found that early minimally invasive ICH evacuation of lobar (superficially located) hemorrhages led to improved functional outcomes compared with medical management alone. However, evacuation of anterior basal ganglia hemorrhages did not prove beneficial (N Engl J Med. 2024;390[14]:1277-1289).
Both the MISTIE III (Lancet. 2019;393[10175]:1021-1032) and MIND (JAMA Neurol. 2025;82[11]:1113-1121) clinical trials failed to show superiority of minimally invasive evacuation techniques over medical management, although signals of improved outcomes were evident in the treatment arms in secondary analyses.
“We need to confirm the positive findings of ENRICH with a larger cohort,” Dr. Bain urges. “In addition, minimally invasive evacuation of hemorrhages in basal ganglia locations is an area that deserves further study.”
Advertisement
Whether the timing of hematoma evacuation contributed to mixed findings in trials assessing craniotomy and minimally invasive techniques needs to be considered. Although evidence indicates a less than 24-hour window yields benefits, ultra-early surgery (e.g., within 8 hours) may be detrimental by risking rebleeding.
“The question of timing may be the most critical factor under our control and has not been rigorously studied,” Dr. Bain says.
Rapid developments in AI are expected to offer important improvements in detecting ICH and characterizing hemorrhage morphology and composition. Combined with advances in imaging, such as diffusion tensor imaging and high-definition fiber tracking, AI should assist with prognosis and the identification of candidates with the greatest chance of recovery from hematoma evacuation.
Technological innovation is also expected to improve intraoperative techniques. The roles of real-time cone-beam CT, phased array ultrasonography and fluorescein for focused cauterization of active bleeding should be evaluated for assessing residual ICH volume during minimally invasive evacuation, which is linked to functional outcome.
In addition, new technologies for minimally invasive access systems are expected to help minimize the surgical footprint while facilitating clot evacuation.
Evidence supporting the importance of early mobilization in the ICU is strong. Efforts need to be standardized and widely implemented.
Improving function in the chronic outpatient phase is being explored with implanted vagus nerve stimulation and epidural cervical stimulation to enhance upper extremity function. Modern remote monitoring technologies to facilitate outpatient care will likely play increasingly important roles in optimizing therapies.
Advertisement
“The ARISE II recommendations provide a good snapshot of large unresolved issues in ICH management,” Dr. Bain concludes. “Most importantly, they provide practical, real-world paths to address them and move the field forward.”
Gabor Toth, MD, an interventional neurologist with Cleveland Clinic’s Cerebrovascular Center, and neurosurgeon Ahmed Kashkoush, MD, a Cleveland Clinic fellow, also participated in the ARISE II effort.
Advertisement
Advertisement

Results may refine surgical selection criteria and advance clinical trial design
ENRICH trial marks a likely new era in ICH management

Digital subtraction angiography remains central to assessment of ‘benign’ PMSAH

Quick and aggressive responses to multiple complications have led to remarkable recovery
Case series links catastrophic outcomes to therapy initiation within 48 hours post-procedure

Scientific program chair reflects on what may resonate longest from this year’s neurosurgery conference

Findings may have implications for understanding the disorders’ pathophysiology

Routine capture of standardized neuroperformance data may expand and refine investigations