Locations:

Vigilance for symptom emergence matters, a large 20-year analysis reveals

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3edd379b-ea77-4939-928f-fdf720a6a74c/HVI_5682658_02-21-25_008_MLC)
doctor explaining a heart model to a patient
Approximately one-quarter of asymptomatic patients with hypertrophic cardiomyopathy (HCM) become symptomatic over long-term follow-up regardless of phenotype, but obstructive HCM is associated with worse long-term survival than nonobstructive disease. Those are leading insights from a 20-year retrospective analysis from Cleveland Clinic, one of the largest studies to date characterizing asymptomatic HCM and its associated long-term outcomes.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The study was presented at the European Society of Cardiology Congress 2025 and simultaneously published by the Journal of the American College of Cardiology.
“These findings highlight the importance of vigilant monitoring of asymptomatic patients with HCM to confirm true asymptomatic status and identify obstructive disease through provocative testing,” says senior author Milind Desai, MD, MBA, Director of Cleveland Clinic’s Hypertrophic Cardiomyopathy Center, who presented the findings. “Such vigilance can help optimize the timing of needed interventions, either preemptively or soon after symptom onset.”
Many patients diagnosed with HCM may remain free of symptoms for long periods. Although current evidence suggests that patients with HCM who are in New York Heart Association (NYHA) class I tend to have a good prognosis and low risk of developing advanced heart failure or mortality related to HCM, these patients’ long-term outcomes are not clear. Likewise, potential variability in outcomes between obstructive and nonobstructive HCM in asymptomatic patients has not been well explored.
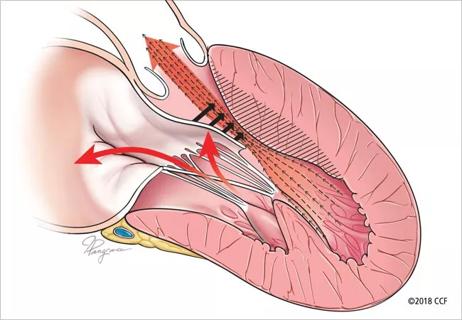
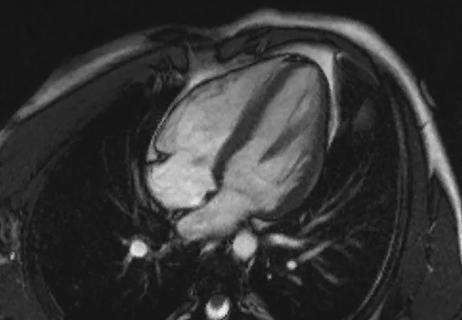
To better characterize outcomes and related factors in this population, Dr. Desai and colleagues retrospectively analyzed 10,143 patients with HCM who underwent extensive clinical and imaging evaluations at Cleveland Clinic from January 2002 to March 2021. Thorough echocardiographic assessment with provocative maneuvers was conducted at baseline and throughout follow-up. HCM was defined as a left ventricular outflow tract (LVOT) gradient of 30 mm Hg or greater at rest or 50 mm Hg or greater with provocation.
Advertisement
Patients’ baseline data were captured from the electronic health record, and NYHA class was determined manually based on individual chart review. Of the overall sample with HCM, 3,393 patients (33.5%) were confirmed to be asymptomatic (NYHA class I) at baseline. These individuals were the focus of the analysis, which noted patients’ NYHA class progression, need for septal reduction therapy, need for heart transplantation and rate of appropriate discharges of implantable cardioverter defibrillators (ICDs) throughout follow-up. The primary endpoint was all-cause mortality, which was determined from medical and public records.
Among the asymptomatic patients, 1,329 (39.2%) had obstructive HCM and 2,064 (60.8%) had nonobstructive HCM. Patients with obstructive HCM were older (mean of 61 vs. 59 years), less often male and more frequently hypertensive, whereas those with nonobstructive disease were more likely to have a family history of HCM and to have an ICD. Atrial fibrillation prevalence was similar between the groups.
Symptom progression. Over mean follow-up of 10.5 years, patients’ symptom profiles were as follows:
Symptom progression rates were similar between patients with obstructive versus nonobstructive HCM.
Interventions. During the study, 11% underwent myectomy (with zero in-hospital mortality), 0.4% underwent alcohol septal ablation, 0.5% received heart transplants and 0.5% experienced appropriate ICD discharges. All patients who underwent septal reduction therapy had developed symptoms before the intervention.
Advertisement
Long-term mortality. Over the mean 10.5-year follow-up, 27% of patients died, with significantly higher mortality among those with obstructive versus nonobstructive HCM (31.8% vs. 24.4%; P < .001). Survival of the patients with nonobstructive disease approximated that of the age- and sex-matched general U.S. population. Survival rates are detailed in the table below.
| Nonobstructive HCM (n = 2,064) | Obstructive HCM (n = 1,329) | |
|---|---|---|
| 5-year survival | 91% | 89% |
| 10-year survival | 80% | 77% |
| 15-year survival | 69% | 64% |
| 20-year survival | 57% | 50% |
| 5-year survival | ||
| Nonobstructive HCM (n = 2,064) | ||
| 91% | ||
| Obstructive HCM (n = 1,329) | ||
| 89% | ||
| 10-year survival | ||
| Nonobstructive HCM (n = 2,064) | ||
| 80% | ||
| Obstructive HCM (n = 1,329) | ||
| 77% | ||
| 15-year survival | ||
| Nonobstructive HCM (n = 2,064) | ||
| 69% | ||
| Obstructive HCM (n = 1,329) | ||
| 64% | ||
| 20-year survival | ||
| Nonobstructive HCM (n = 2,064) | ||
| 57% | ||
| Obstructive HCM (n = 1,329) | ||
| 50% |
Independent predictors of higher long-term mortality were older age, female sex, history of atrial fibrillation and obstructive (vs. nonobstructive) HCM (P < .001 for all on multivariable analysis). Medication use did not influence survival outcomes.
“We found that slightly more than a quarter of asymptomatic HCM patients developed symptoms over time, and this rate was the same for both obstructive and nonobstructive phenotypes, yet obstructive HCM was associated with significantly worse long-term survival,” Dr. Desai observes. “These findings align with results from smaller prior studies, which bolsters their strength.”
He adds, however, that they demonstrate association, not causation, due to the study’s observational nature, and that prospective validation would be welcome.
“Nevertheless, these results make a strong case for diligent assessment of HCM patients for obstructive physiology and for true symptom-free status,” Dr. Desai continues. “This can be done using provocative measures, including exercise stress testing.”
While evidence is lacking for pharmacotherapies for asymptomatic HCM, the authors note that the finding of worse long-term survival in asymptomatic patients with obstructive HCM may provide a rationale for studying earlier initiation of disease-modifying therapies in this population.
Advertisement
And while septal reduction therapy is not recommended for asymptomatic patients with obstructive HCM, the authors note that only 12% of the longer-term deaths in patients with obstructive HCM occurred in patients who had a myectomy (52 of 422 deaths), much lower than the 27% of patients with obstructive HCM overall who underwent myectomy (361 of 1,329 patients).
“This suggests that timely septal reduction therapy in previously asymptomatic patients, when performed at high-volume centers, may have a protective effect,” says co-author Nicholas Smedira, MD, MBA, Surgical Director of the Hypertrophic Cardiomyopathy Center. “The argument for vigilance around early symptom detection in this population is clear.”
Advertisement
Advertisement

End-of-treatment VALOR-HCM analyses reassure on use in women, suggest disease-modifying potential

Cardiac imaging substudy is the latest paper originating from the VANISH trial

Phase 3 ODYSSEY-HCM trial of mavacamten leaves lingering questions about potential broader use

5% of flagged ECGs in real-world study were from patients with previously undiagnosed HCM

High composite score in myectomy specimens signals worse prognosis
Few patients report left ventricular dysfunction or heart failure after one year
Avoidance of septal reduction therapy continues while LVEF dysfunction remains infrequent

New risk score pools factors that may predict adverse outcomes in the uncommon phenotype