Locations:

From dryness to diagnosis

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/039db37a-191b-43a4-a5e7-e30a9ee90ef7/case-study-IgG4-feature)
Patient with swollen throat
By Komal Ejaz, MD, and Ambreesh Chawla, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
IgG4-related disease is a rare autoimmune condition that affects multiple organ systems, including the salivary and lacrimal glands, thyroid gland, pituitary gland, pancreas, biliary tree, aorta, breast and other organs.1 In most cases, if one organ system is found to be involved, screening for additional organ involvement is prudent.
Here we discuss a case of IgG4-related disease in 67-year-old female, for whom additional screening revealed multisystem involvement.
The patient was referred to Rheumatology due to concerns for Sjögren’s disease because of Sicca symptoms and glandular enlargement. She presented after noticing gradual onset swelling of her neck without any associated pain. Her medical history was notable for endometrial clear-cell adenocarcinoma (status post-surgical resection and chemotherapy), osteoarthritis, hypertension, epilepsy and migraines.
An initial computed tomography [CT] scan of her neck showed bilateral enlarged submandibular glands with no ductal dilatation or submandibular stones. She was referred to Otolaryngology, and a submandibular massage was performed. This slightly improved her swelling, but it returned within a week.
The patient later noted new symptoms of dry eyes and dry mouth. Because of her Sicca symptoms and the persistence of submandibular swelling, she was referred to Rheumatology for evaluation for Sjögren’s disease.
During the initial Rheumatology visit, the patient was found to have elevated ESR of 49 mm/hr and C-reactive protein of 1.8 mg/dL. Given the Sicca symptoms and glandular swelling, lupus and Sjögren’s syndrome were considered, but the workup showed negative anti-nuclear antibody (ANA) and extractable nuclear antigen (ENA). Rheumatoid factor was 17 with a negative anti-cyclic citrullinated peptide (anti-CCP).
Advertisement
Further workup revealed an IgG total of 2009 mg/dL and IgG4 subclass at 535 mg/dL. The patient’s IgE level was high at 626 kU/l, complement 3 (C3) was high at 224 and complement 4 (C4) was high at 49. She was referred for fine-needle aspiration of the right submandibular gland, which showed a polymorphous population of lymphoid cells with scattered plasma cells; staining for CD138 and IgG4 was suboptimal.
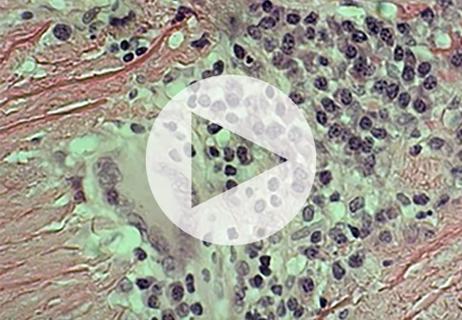
The patient continued to report worsening submandibular swelling [top image] and was referred for an incisional biopsy of the submandibular gland. This revealed chronic sclerosing sialadenitis with marked fibrosis in a perilobular pattern, dense lymphoplasmacytic infiltrate, and polyclonal plasmacytosis. Most of the plasma cells stained positive for IgG and the majority were positive for IgG4 (171 IgG4-positive plasma cells per high power field seen; IgG4:IgG ratio = 105%).
CT imaging of the patient’s chest revealed pulmonary nodules and axillary lymphadenopathy. Imaging of her abdomen revealed a 22.4 mm x 18.1 mm soft-tissue lesion between the proximal common iliac arteries, eccentric soft-tissue thickening along the left anterolateral wall of the abdominal aorta, and mild infiltration adjacent to the distal abdominal aorta, which was concerning for retroperitoneal fibrosis (Figure 3). Subtle haziness adjacent to the pancreatic tail was also seen, which raised the possibility of autoimmune pancreatitis.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/03508c62-202c-44d8-8b1e-7d701765c00e/case-study-IgG4-inset2)
Figure 3. CT abdomen showing a 22.4 mm x 18.1 mm soft tissue lesion between the proximal common iliac arteries, eccentric soft tissue thickening along the left anterolateral wall of the abdominal aorta, and mild infiltration adjacent to the distal abdominal aorta concerning for retroperitoneal fibrosis.
The patient was diagnosed with IgG4-related disease and started on prednisone 40 mg along with rituximab. Two infusions of 1 gram of rituximab were given two weeks apart. Prednisone was tapered slowly over the next four months.
Advertisement
Within two months, the patient’s IgG4 levels normalized to 55.8 mg/dL. She had almost complete resolution of submandibular gland swelling [Figure 2].

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/aa2cef8b-4cbb-49bc-9a53-a99c0ab89335/case-study-IgG4-inset1)
Figure 2: The neck swelling resolved after treatment.
CT imaging of her abdomen after treatment showed decreased soft-tissue thickening caudal to the aortic bifurcation and along the left lateral inferior wall (Figure 4) with interval atrophy of pancreatic body and tail corresponding with clinical response.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/bfde41e1-2bde-4058-95f9-f654a18ff013/case-study-IgG4-inset3)
Figure 4: CT abdomen showed interval decrease in size of soft tissue thickening caudal to the aortic bifurcation and along the left lateral inferior wall.
Discussion
Histopathologic findings of IgG4-related disease are similar irrespective of the involved organ system. They include lymphoplasmacytic infiltrate, obliterative phlebitis, storiform pattern fibrosis, and the presence of IgG4-positive plasma cells with IgG4/IgG ratio >40% and total IgG4 plasma cells > 10/high power field.1
While elevated plasma IgG4 levels can be a helpful indicator, it is important to note that they are neither sensitive nor specific for diagnosis of IgG4-related disease, and pathology remains the gold standard.2 Normal IgG4 levels have been reported in nearly a quarter of cases.3
Other pertinent findings include eosinophilia, elevated IgE levels, high circulating plasmablasts, and low C3 and C4, particularly with renal involvement.
Clinical observation is often sufficient for patients with asymptomatic IgG4-related disease. Even mild lymphadenopathy and submandibular gland swelling can be longitudinally followed.
However, glucocorticoids are the mainstay of therapy in cases with multisystem or severe involvement, such as in our patient with impressive submandibular gland swelling, retroperitoneal fibrosis, and potential pancreatic involvement.
Advertisement
While response is typically quick with glucocorticoids, tapering is often linked to disease relapses.2 This is where steroid-sparing agents are considered, and medications — including methotrexate, mycophenolate, azathioprine and cyclophosphamide — have been used.4 Emerging data indicate both clinical and laboratory improvement in IgG4 levels and circulating plasmablasts may be seen with rituximab in IgG4-related disease.5 In some cases, a single cycle is sufficient, although maintenance therapy may be needed and there is a high risk of relapse or organ dysfunction.
Advertisement
1. Khosroshahi, A., Carruthers, M. N., Deshpande, V., Unizony, S., Bloch, D. B., & Stone, J. H. (2012). Rituximab for the treatment of IgG4-related disease: lessons from 10 consecutive patients. Medicine, 91(1), 57-66.2.
2. Al-Khalili, O. M., & Erickson, A. R. (2018). IgG-4 related disease: an introduction. Missouri medicine, 115(3), 253.
3. Sekiguchi, H., Horie, R., Kanai, M., Suzuki, R., Yi, E. S., & Ryu, J. H. (2016). IgG4‐related disease: retrospective analysis of one hundred sixty‐six patients. Arthritis & Rheumatology, 68(9), 2290-2299.
4. Khosroshahi, A., Wallace, Z. S., Crowe, J. L., Akamizu, T., Azumi, A., Carruthers, M. N., ... & Stone, J. H. (2015). International consensus guidance statement on the management and treatment of IgG4‐related disease. Arthritis & rheumatology, 67(7), 1688-1699.
5. Carruthers, M. N., Topazian, M. D., Khosroshahi, A., Witzig, T. E., Wallace, Z. S., Hart, P. A., ... & Stone, J. H. (2015). Rituximab for IgG4-related disease: a prospective, open-label trial. Annals of the rheumatic diseases, 74(6), 1171-1177.
Advertisement

Evidence suggests empathy influences immune function and well-being

Going beyond simple referrals to streamline patient access

Cleveland Clinic group works toward earlier diagnosis of this rare disease

New clinic meets Hispanic patients where they are

Fellows will train under faculty with broad range of expertise

Collaboration was key to identifying source of nerve condition
When to suspect concurrent giant cell arteritis

New research explores the role of immune cell and blood-brain barrier changes