Locations:

Enhanced visualization and dexterity enable safer, more precise procedures and lead to better patient outcomes

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e4b8364c-a8e6-4e87-9dae-b5fa39bc8ba3/pita-robotic-1)
physicians in operating room
Cleveland Clinic has added another milestone to its long history of innovation in transplantation. In mid-November 2025, Alejandro Pita, MD, Director of Living Donor Liver Transplantation, led a multidisciplinary team in performing the institution’s first fully robotic liver transplant, encompassing both hepatectomy and implantation
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“It is quite an achievement for the entire team,” notes Dr. Pita. “This operation has historically been one of the defining examples of open surgical technique. To complete it robotically is remarkable.”
While robotic liver transplantation remains limited to only a handful of centers worldwide, its potential advantages are significant. The robotic approach minimizes muscle disruption and reduces postoperative discomfort.
“There is less surgical pain because the incision is smaller and does not split muscle,” Dr. Pita explains. He adds that existing evidence supports these benefits: “Studies show that minimally invasive approaches, laparoscopic and robotic, lead to less intraoperative blood loss, fewer complications, faster recovery, and improved cosmetic outcomes compared to open surgery.”
The robotic system also enhances technical precision. Dr. Pita notes that the platform’s 3D, high-magnification visualization and wristed instruments provide superior maneuverability during the most delicate steps of transplantation, including vascular and biliary anastomoses.
These advantages made the approach particularly compelling for the patient involved in this historic case, whose clinical stability and anatomy aligned well with the demands of a fully robotic procedure. As Dr. Pita explains, thoughtful patient selection is essential when introducing a new modality—setting the stage for the team’s decision-making process and the patient’s path to transplant.
The recipient of this landmark procedure was a middle-aged woman with cirrhosis secondary to primary biliary cholangitis (PBC). As Dr. Pita explains, “This disease can affect patients and lead to a series of complications that ultimately make liver transplantation necessary,” and the patient had been listed for transplant before receiving the deceased-donor organ offer.
Advertisement
Because fully robotic liver transplantation remains highly specialized and technically demanding, patient selection is deliberate and multifactorial. Dr. Pita notes that candidates must be medically stable enough to tolerate a longer operation. “Ideally, the patient is not extremely sick,” he says. Patients who require high-dose medications to maintain blood pressure or who fall at the severe end of the illness spectrum are typically not appropriate candidates at this stage.
Anatomy also plays a critical role. “Selection is highly technical and anatomical,” Dr. Pita explains, while noting that adequate working space within the abdomen is necessary—sometimes aided by the presence of ascites—and a smaller native liver is preferable to allow safer and more efficient dissection. Donor organ quality is similarly important, as the graft must tolerate a potentially longer implantation time associated with the robotic approach. The application of adjunct perfusion techniques, including normothermic regional perfusion in the donor followed by ex-vivo normothermic machine perfusion, allowed for the safe use of a donation after circulatory death (DCD) graft, traditionally considered an extended-criteria organ.
Surgical history factors into the equation as well. “We initially avoid patients with multiple prior abdominal surgeries or those undergoing re-transplantation,” Dr. Pita says. For this patient, the combination of clinical stability, favorable anatomy, and a high-quality donor organ made her an excellent candidate. These considerations, combined with extensive team preparation, helped create the conditions necessary for the transplant to proceed safely and successfully.
Advertisement
With patient selection confirmed, the team proceeded to plan and execute the fully robotic transplant. “Because this was a first-of-its-kind procedure, months of preparation went into designing workflows, anticipating challenges, and practicing on cadavers,” Dr. Pita says. The meticulous planning ensured that every step—from donor liver arrival to vascular and biliary anastomoses—could be performed safely using the robotic platform.
“This case involved a deceased-donor liver transplant,” he continues. Once the donor organ was transported to the hospital, the recipient was brought to the operating room under general anesthesia. Unlike traditional open transplantation, which requires a large upper-abdominal incision, the robotic approach uses multiple small port sites along with a limited extraction incision.
“We make several small incisions and dock the robot through a series of ports,” Dr. Pita outlines. “The robot includes a camera and specialized instruments that allow us to operate within the abdomen, which is inflated with CO₂ to establish pneumoperitoneum.”
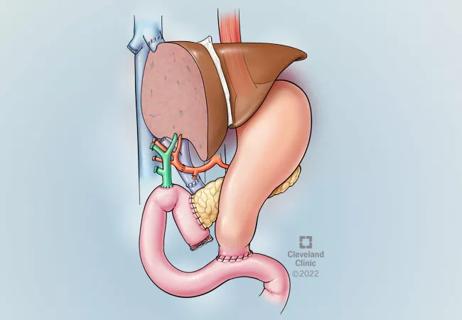
From the surgeon’s console, Dr. Pita controlled the articulated robotic instruments while receiving three-dimensional, high-magnification visualization. This setup allows precise dissection and the creation of delicate vascular and biliary connections. “During surgery, four key anastomoses are created: the cavocavostomy, portal vein, hepatic artery, and bile duct. All of these are completed robotically,” he notes. The enhanced dexterity and stability of the robotic instruments make these steps technically more feasible than with laparoscopic tools, particularly in tight anatomical spaces.
Advertisement
Team coordination was critical to the operation’s success. Bedside assistance, skillfully provided by Dr. Jaekeun Kim, Dr. Mazhar Khalil, and surgical fellows Sami Shoucair and Woo Jin Choi supported instrument exchange, retraction, and workflow management, while surgical nurses ensured seamless logistics, instrument readiness, and optimal operating room layout. “A tremendous amount of credit goes to our surgical nursing team, who assembled instruments, coordinated logistics, planned operating room layouts, and prepared everything necessary for that day,” Dr. Pita says. “It truly is a collective effort.”
Following the operation, the patient demonstrated a smooth recovery. “She is doing well and went home,” Dr. Pita reports. Although the team returned briefly to the operating room to evaluate the hepatic artery, this intervention did not affect her overall outcome. Remarkably, she was discharged two days earlier than the length of stay typically observed after open liver transplantation at Cleveland Clinic.
Dr. Pita notes that her prior history of chronic pain would normally complicate postoperative management, making her rapid recovery an important indicator of the robotic approach’s benefit. “The fact that she recovered well and was discharged earlier than average highlights the lower postoperative pain associated with minimally invasive approaches.”
Postoperative care for robotic transplant recipients remains consistent with standard protocols. Patients are seen at two weeks, three weeks, six weeks, three months, six months, and one year, with close monitoring for immunosuppression, graft function, and complications. “Follow-up is identical to standard transplant care,” Dr. Pita explains. The robotic modality does not require additional surveillance or adjustments to clinical pathways.
Advertisement
The implications of this procedure extend beyond individual patient outcomes. Robotic liver transplantation is technically demanding, and its adoption has been limited to only a few centers worldwide. “This represents the new frontier of liver transplantation,” Dr. Pita says. He notes that robotic kidney transplantation has been performed for longer, but the complexity of liver anatomy makes robotic liver transplantation uniquely challenging.
Cleveland Clinic’s accomplishment highlights both innovation and institutional support. The team initially began with robotic living donor hepatectomy, progressed to hybrid recipient operations, and, after five successful hybrid cases, performed this case—their first fully robotic transplant. “The benefit is being at the forefront of innovation and providing patients with improved outcomes while advancing the field of transplantation,” Dr. Pita shares.
Beyond technical milestones, the procedure offers tangible patient-centered advantages. Robotic surgery reduces incision size, muscle disruption, and postoperative pain, while improving visualization, precision, and cosmetic outcomes. Shorter hospital stays and fewer complications may become more routine as centers gain experience. Dr. Pita emphasizes, “The ultimate goal—whether for donors or recipients—is minimizing incisions and improving outcomes while maintaining safety.”
By joining a small group of U.S. and international institutions performing fully robotic liver transplants, Cleveland Clinic sets a benchmark for safe advancement in transplantation. The team’s experience demonstrates that with careful patient selection, detailed planning, and a highly coordinated multidisciplinary approach, robotic liver transplantation can expand the boundaries of surgical care.
Advertisement

A surge in transplants, advanced surgical techniques and multidisciplinary collaboration has helped shape and expand the Liver Transplant Program

Minimally invasive approach, peri- and postoperative protocols reduce risk and recovery time for these rare, magnanimous two-time donors

Patient receives liver transplant and a new lease on life

New research shows dramatic reduction in waitlist times with new technology

Cleveland Clinic study shows positive outcomes for donors and recipients

Program's approach maximizes donor safety without compromising recipients' outcomes

Program expands as data continues to show improved outcomes
Atypical cells discovered after primary sclerosing cholangitis diagnosis