Locations:

Guidance from the largest cohort of SEEG-confirmed insular epilepsy patients reported to date
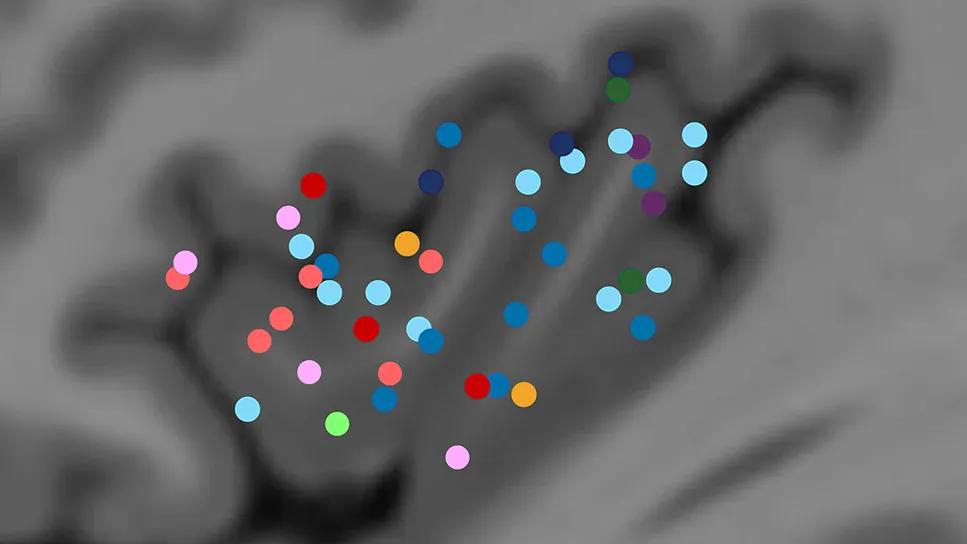
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9e35ea73-6308-48da-a672-6a2a69f2c4f0/brain-scan-with-added-color-dots)
brain scan with colored dots over a dark gray region
Identifying the source of seizures in the insular cortex has long been a leading challenge in epilepsy surgery. Because of its deep location and extensive connections, the insular lobe can produce clinical signs that mimic other brain regions, often leading to surgical failures. However, a new Cleveland Clinic study published in Annals of Neurology (2025;98:1111-1124) provides clinicians with a clearer roadmap for identifying possible insular epilepsy and distinguishing between anterior and posterior seizure onset.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Our primary finding is that the type of aura or absence of aura and the temporal progression of clinical signs are highly predictive of the seizure onset zone,” says lead and corresponding author Jason Chisholm, MD, a neurologist in Cleveland Clinic’s Epilepsy Center. “For example, the absence of an aura strongly suggests an anterior insular onset, whereas unilateral nonpainful somatosensory sensations frequently indicate a posterior origin. These insights can help clinicians refine diagnostic hypotheses and optimize stereoelectroencephalography [SEEG] implantation strategies.”
The insula is a complex, eloquent structure involved in various functional systems, including sensorimotor, limbic and interoceptive domains. Its intricate architecture, transitioning from an agranular anterior zone to a granular posterior zone, contributes to a wide range of seizure manifestations. “Historically, insular seizures have been difficult to identify because they frequently imitate temporal, frontal or parietal lobe epilepsy,” Dr. Chisholm explains.
In the current study, he and colleagues analyzed the largest cohort of SEEG-confirmed insular epilepsy patients reported to date, comprising 45 individuals evaluated at Cleveland Clinic’s Epilepsy Center from 2009 to 2021. The difficulty of diagnosing this condition is reflected in the fact that 44.4% of the patients had undergone a prior, unsuccessful resection before the insula was identified as the true culprit. Furthermore, noninvasive tests often fall short; for example, scalp EEG failed to show epileptiform discharges in nearly one-third of the patients.
Advertisement
To provide a more granular understanding of the insula, the researchers used an MRI-based anatomical framework to divide the lobe into six subdivisions, with the anterior insula consisting of four subdivisions (anterior inferior cortex and three short gyri [anterior, middle and posterior]) and the posterior insula consisting of two subdivisions (anterior and posterior long gyri).
They meticulously reviewed 440 seizure videos from the 45 patients, documenting 94 distinct clinical manifestations and their exact timing.
The team then correlated these signs with SEEG data to determine whether specific behaviors emerged early (within the first third of the seizure) or late. “This temporal analysis is crucial, as it reflects how the epileptic activity spreads through the brain’s networks,” Dr. Chisholm notes.
One of the study’s most significant findings is what the researchers call an “anterior-to-posterior gradient” observed in aura types. Auras were reported by 87% of the cohort (39 of 45 patients), making them a vital diagnostic marker. Among the key findings:
Advertisement
Beyond auras, the study identified several objective signs that can help differentiate the two regions in terms of seizure onset, with timing of the signs playing an important role.
Findings suggestive of anterior onset included late-emerging grunting or moaning, symmetric mouth movements, repetitive blinking, and chewing or swallowing behaviors. Additionally, early tachycardia was strongly associated with the middle short gyrus.
Findings suggestive of posterior onset were early elementary motor signs in the hand or arm, axial tonic posturing and bilateral asymmetric tonic posturing.
The researchers also found that certain signs tend to co-occur. For instance, cognitive auras were frequently followed by restlessness, hyperkinetic movements and autonomic features such as hypersalivation or hyperventilation.
The study reinforces the safety and efficacy of modern surgical approaches for insular epilepsy. SEEG exploration, using both orthogonal and oblique electrode trajectories, resulted in no complications across the 45 patients.
Following SEEG, 39 patients proceeded with surgical treatment, including resection and laser interstitial thermotherapy (LITT). Results were encouraging:
Advertisement
“These findings suggest that the insula should be reconsidered when a patient’s seizure semiology is atypical, when it includes a distinct aura or when previous surgeries have failed,” Dr. Chisholm observes.
He and his co-authors note that their study also underscores the importance the clinical interview can have in ascertaining the presence, nature and timing of an aura.
“Although additional larger studies of the semiology of insular epilepsy are needed, insights from this study can help clinicians better advocate for targeted SEEG evaluations in the knowledge that focal curative treatment for insular epilepsy is not only feasible but increasingly successful,” Dr. Chisholm concludes.
Image at top: A map of aura distribution by seizure onset zone. Reprinted from Chisholm et al., Annals of Neurology (2025;98:1111-1124), under the Creative Commons Attribution--NonCommercial license.
Advertisement
Advertisement

Data-driven segmentation approach shows promise for seizure characterization with utility for clinical decision making

Systematic review indicates more can be done for higher-risk patients

Insights from one of the first studies of invasive monitoring in the rare form of focal cortical dysplasia

A case study in pairing imaging acumen with subspecialty expertise to yield answers and symptom relief

Despite less overall volume loss than in MS and NMOSD, volumetric changes correlate with functional decline

Researchers pair quantitative imaging with AI to improve surgical outcomes in nonlesional epilepsy

Despite advancements in the specialty, patient-centered care needs to remain a priority

Promising preclinical research indicates functional motor recovery is durable