Locations:

Cleveland Clinic reports first U.S. series focused on use in this challenging setting
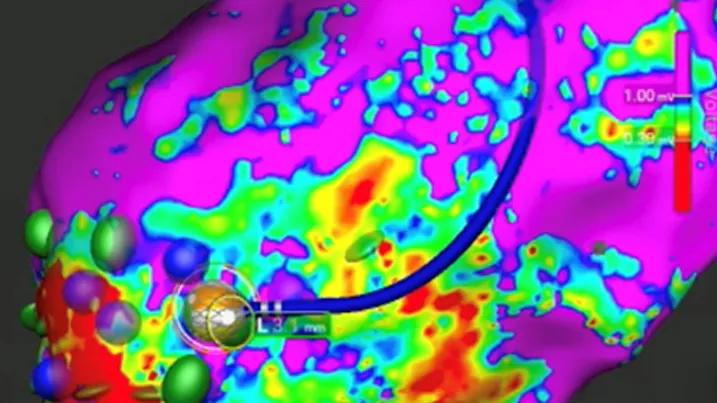
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a5a6bb06-cdf6-4557-b659-03fa40f15e1c/dual-energy-ablation-VT)
map of the heart for use in cardiac ablation with catheter atop the map
The first U.S. series reporting on ablation of ventricular arrhythmias (VAs) with a dual-energy lattice-tip catheter shows the approach to be effective, efficient and generally safe. The 59-patient Cleveland Clinic series — presented in a late-breaking clinical trials session at the Heart Rhythm Society’s Heart Rhythm 2026 meeting and simultaneously published in JACC: Clinical Electrophysiology — evaluated procedural and clinical outcomes of VA ablation with a wide-footprint catheter that can toggle between radiofrequency ablation (RFA) and pulsed field ablation (PFA).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Ablating ventricular arrhythmias with a lattice-tip RFA/PFA catheter was associated with good procedural success and favorable mid-term outcomes,” says the report’s senior and corresponding author, Pasquale Santangeli, MD, PhD, Director of the Ventricular Tachycardia Program at Cleveland Clinic. “Our findings also revealed a need for caution when PFA is delivered near exposed implanted cardiac device conductors, when the catheter is maneuvered near the mitral or tricuspid valves, and when epicardial mapping may risk the trapping of fat within the catheter sphere. This early experience is encouraging, but further use and investigation will be required to optimize PFA parameters for use in ventricular substrates.”
Small solid-tip RFA catheter ablation has been the standard for treating recurrent refractory VAs for more than a quarter century, but the approach has limitations, including a small footprint and depth penetration insufficient for some cases, especially those involving complex scars.
In the context of these limitations, proceduralists saw potential when a wide-footprint catheter with a spherical lattice tip and the ability to deliver both RFA and PFA energy was commercially approved in late 2024 (Sphere-9™ catheter, Medtronic). Although the approval was for catheter ablation of atrial fibrillation, the catheter’s ability to create larger lesions than standard small-tip RFA catheters spurred interest in application to challenging VA substrates.
“This interest was bolstered by preclinical ventricular arrhythmia studies, including at Cleveland Clinic, showing larger lesions than with conventional RFA catheters and the ability to achieve deeper, more uniform lesions with this catheter’s PFA setting,” Dr. Santangeli notes.
Advertisement
Despite early exploration of the new catheter’s utility for targeting VA substrates, no U.S. centers had reported on its use in this setting prior to the current study.
To fill this gap, Dr. Santangeli and colleagues evaluated their early experience with the strategy for VAs from the prospectively maintained Cleveland Clinic CLEAR-VT Registry. Specifically, they analyzed outcomes of 59 consecutive patients who underwent ablation for VA — either ventricular tachycardia (VT) or premature ventricular contractions (PVCs) — between January and September 2025 using the dual-energy lattice-tip catheter.
“The decision to use this catheter in this setting was based on patients either having an anticipated large target substrate area, indicated by multisegment scar involvement on imaging, or prior failure of conventional RFA,” explains Cleveland Clinic electrophysiologist Jakub Sroubek, MD, PhD, a co-author of the series report.
The ablation strategy involved a sequential protocol using high-density substrate mapping, with RFA serving as the first-line ablation modality followed by toggling to PFA for adjunctive ablation in areas with dense scar. PFA was avoided near the substrate border zone.
The patients were a relatively high-risk, complex group:
Advertisement
Outcomes showed ablation with the catheter to be generally effective and efficient.
Among patients with VT (n = 50):
Among patients with PVCs (n = 9):
Procedures were fairly short for ablation in this complex setting, with a mean duration of 185 minutes for VT and 118 minutes for PVCs.
Overall complication rates were low. There was no evidence of coronary vasospasm or signs of hemolysis, but three major procedure-related complications occurred: two major bleeding events and one failure of an implantable cardioverter-defibrillator (ICD) system. The bleeds were periprocedural hemorrhagic complications that were not device-related. The ICD system failure occurred after PFA was delivered about 7.5 mm away from a left ventricular pacing lead, requiring generator replacement that was successfully completed during the procedure.
The authors identify the ICD failure as an important cautionary finding of the series, emphasizing the need for care when using PFA near exposed conductors of implanted cardiac devices.
Advertisement
In addition to the caution relating to implanted devices, the authors shared several other practical observations from their early experience:
“While our early experience with this technology in patients with ventricular arrhythmias is promising, it also has yielded practical insights for reducing procedural risks and identified opportunities to further optimize PFA parameters to improve lesion depth,” Dr. Sroubek observes.
“Because this series employed uniform procedural approaches and follow-up protocols, it helpfully builds on previous findings from the multicenter European VA ablation registry, which captured heterogeneous ablation techniques and follow-up protocols,” adds Dr. Santangeli.
Advertisement
“Further study is needed to evaluate whether this dual-energy platform enhances long-term outcomes relative to conventional approaches to VA ablation,” he continues. “For now, the acute and midterm outcomes we’ve observed to date are comparable or numerically superior to those in contemporary reports of substrate-based VT ablation with conventional RFA, with meaningfully shorter procedure time thanks to the catheter’s broad-footprint design and lack of need to exchange catheters. That is an encouraging finding.”
Image at top reprinted from Dasa et al., JACC: Clinical Electrophysiology, under the Creative Commons CC BY license.
Advertisement

Experts discuss advances in precision medicine, the value of collaborative care and more

Application to flutter found safe and effective in study of 300+ patients

Study identifies a cohort of low-risk patients, finds LVEF predicts late VT/VF in those at higher risk

Nonthermal method promises faster procedure times, less risk to adjacent structures

CMR-CLIP outperforms general AI tools; may one day expand patient access to CMR

Large series confirms early and long-term survival advantages over partial pericardial resection

AVANT GUARD trial extends first-line role for ablation beyond paroxysmal atrial fibrillation

Intracardiac echo mapping of para-septal fat pads provides fast, accurate and radiation-free targeting