Locations:

Early detection, prognostication and intervention may improve outcomes
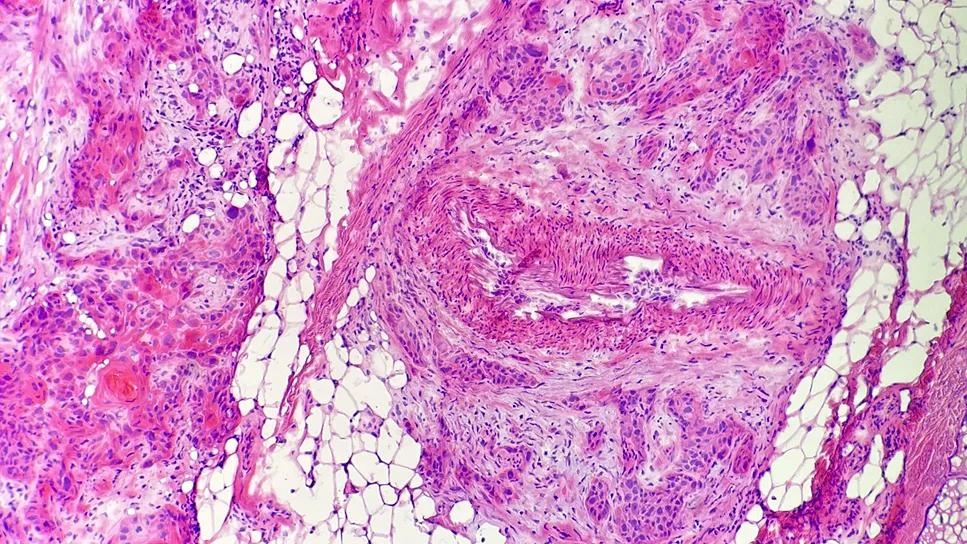
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/661b42d6-3433-46f2-b434-e4440a64951c/radiologic-imaging-helping-treat-cutaneous-scc)
Squamous cell carcinoma
Lymphovascular invasion (LVI) is not part of the two most commonly used squamous cell carcinoma staging (cSCC) systems. However, this invasion of cancer to the blood vessels and/or lymphatics is an independent predictor of metastasis and disease-specific death, according to a major international study. The findings were published in the Journal of the American Academy of Dermatology.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“The Brigham & Women's (BWH) and American Joint Committee on Cancer (AJCC) staging systems do a good job of predicting outcomes for cutaneous squamous cell carcinoma. However, we believe that we can improve on prognosticating to determine which tumors need more aggressive treatment,” says study co-author Allison T. Vidimos, RPh, MD, a dermatology specialist with Cleveland Clinic Cancer Institute.
CSCC usually is highly treatable with favorable outcomes, but in a small percentage of cases, patients who have high-risk features such as poorly differentiated histopathology, deep invasion or perineural invasion (PNI) do not fare as well. LVI is rare, so to date it’s been unclear what its full impact is on patient outcomes.
LVI can be elusive and difficult to identify on histopathology. Typically, Mohs surgeons check the edges of the excision of a cSCC tumor to confirm they’ve removed all abnormal cells, but LVI may be at the center of the tumor (i.e., the nonmarginal skin) and therefore may be missed using this approach.
“If we don't know that squamous cell carcinoma has invaded the blood or lymphatic vessels, we're not going to be prompted to do imaging or lymph node sampling,” says Dr. Vidimos. “We’ll have a false sense of security that the cancer is all out, when LVI could be lurking in the nonmarginal tissue, which can portend a more aggressive tumor.”
As new therapies such as the immunotherapy cemiplimab have received FDA approval for treating patients with locally advanced or metastatic cSCC who are not candidates for curative surgery or curative radiation, it’s become even more important to identify patients early on who may be candidates for more extensive evaluation, aggressive treatment and closer follow up.
Advertisement
LVI had already been identified as a predictor of cSCC-specific death in small cohorts. Building on this work, Cleveland Clinic Cancer Institute and Brigham & Women’s Hospital initiated a retrospective analysis of patients with cSCC who were treated at various academic and regional medical centers. Their work became the largest retrospective study assessing the role of LVI in disease outcomes.
“There’s power in numbers,” says Dr. Vidimos. “The more tumors we evaluate in different practice settings, the better we can determine how best to treat patients.”
Ten practices in the U.S., one in Spain and one in Brazil participated in the research, sharing de-identified patient data, including:
The collective database represented 23,166 tumors from 14,825 patients. The researchers used means, medians and interquartile analysis of the statistics. They assessed associations between relevant variables and LVI status, taking into account patients with multiple tumors.
In addition to participating in the study, the researchers in this cSCC consortium regularly meet to share data and insights. "It's uplifting to see how generous our collaborators are with their time," says Dr. Vidimos. "Everyone is working together to figure out how to optimally treat these cSCC patients. That's been a real gift to all of us and the patients we serve."
Advertisement
Although LVI tumors were rare (representing 7.7% of all tumors in the collective database), patients who had these had an 82% increase in poor outcomes, including three times the risk of local recurrence and ten times the risk of metastasis and disease-related death compared to non-LVI tumors. Patients with LVI+ tumors were also more likely to have nodal positivity after lymphadenectomy compared to those with LVI- tumors. “Even in patients with only one worrisome feature, that single finding of LVI made the outcome much worse,” says Dr. Vidimos.
These findings were consistent across low- and high-grade BWH tumors. Low-stage BWH tumors (T1 or T2a) that were LVI+ had poorer outcomes compared to low-stage BWH tumors (20.8 vs. 1.61% at three years) that were LVI-. There were no notable differences in sex, age or immunocompromised status between the LVI+ and LVI- groups.
Analysis of baseline imaging showed that 12.3% of LVI+ tumors showed metastases compared to 1% of LVI- tumors. “Nearly 40% of LVI+ tumors were classified as low BWH stage and over 20% of those tumors had a major poor outcome at a three-year follow-up, emphasizing that LVI inclusion as a high-risk variable in staging systems would upstage a significant portion of LVI+ tumors with prognostic implications,” the study authors noted.
These findings demonstrate the importance of performing advanced imaging at baseline as well as regular surveillance in cSCC cases with LVI.
Dr. Vidimos noted some limitations of the study, including variability in clinical practice across centers. Additionally, detecting LVI in frozen sections and on permanent histology sections is a challenge. This may have led to underreporting.
Advertisement
To help with identification of high risk cSCC patients to optimize evaluation, treatment and follow up, this cSCC data was used to develop a free app called riSCC. Clinicians enter a patient’s age; gender; immunosuppression status; tumor location, size and differentiation; tumor depth; presence of PNI or LVI and whether the cSCC is recurrent or not. The app then calculates the probability that the tumor will recur locally, develop in-transit metastases, metastasize to the lymph nodes or to distant sites or cause disease-specific death following Mohs surgery or excision.
This study revealed several recommendations for improving diagnosis and treatment, including:
Proactively looking for LVI. At Cleveland Clinic, Mohs surgeons send a sample of the nonmarginal tissue of high-risk CSCC tumors to pathology to check for concerning features such as LVI and PNI that may prompt additional imaging, adjunctive treatment and closer follow up. If further treatment is warranted, the patient may receive adjuvant radiation or immunotherapy following surgery based on imaging and pathology of metastases.
Seeking guidance from a radiologist to choose the appropriate imaging study to identify PNI and metastatic spread. “Radiologists can assist in the choice of the optimal imaging study (e.g., MRI, CT, PET CT or ultrasound) and protocol the imaging studies to better see what you’re asking them to look for, such as PNI, bone invasion, lymph node spread or distant tumor spread,” says Dr. Vidimos.
Providing insight to the radiologist about clinical concerns when ordering scans. “Sometimes abnormal radiologic findings are very subtle, so it’s crucial to share any clinical suspicions that will help the radiologist make an accurate interpretation,” says Dr. Vidimos. In one study, subtle perineural invasion was missed on imaging studies 79% of the time when radiologists weren’t prompted to look for it. To that end, it is essential to communicate the location of the tumor; prior treatments; and pertinent concerning history, histologic or clinical findings (deep tumor invasion, LVI, PNI, sensory or motor nerve deficits and/or significant physical exam findings).
Advertisement
Based on the study outcomes, there is a need to refine the current cSCC staging systems for improved prognostication, which is in process by the cSCC consortium. In addition, the research team is performing a validation study for the riSCC app.
Advertisement

A proactive, framework-based approach

Patients on ibrutinib were more than twice as likely to experience atrial fibrillation or heart failure than those on second-generation alternatives.

Expert recommendations introduce use of targeted agents

Combination therapy may soon represent new standard of care

Research findings offer clues for improving disease outcomes in men

Creating a safe space for patients

Long-term immune effects reshape preventative strategies and timelines

Large-scale database also reveals potential for immunotherapy to protect against cancer