Locations:

Women’s Comprehensive Health and Research Center addresses unmet needs

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/63dd1257-30fb-42a4-8b04-4024fed14bf8/womens-health-research)
Dr. Batur examining patient
To enhance healthcare for women at midlife and beyond, Cleveland Clinic has launched its Women’s Comprehensive Health and Research Center with a mission to increase patient access, build connectivity among medical specialties, improve education and expand research to transform patient care.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The Women’s Comprehensive Health and Research Center, which opened in April 2024, was developed by Cleveland Clinic leaders and Maria Shriver, journalist and advocate, who serves as its chief visionary and strategic partner. Shriver is also the founder of Women’s Alzheimer’s Movement (WAM) at Cleveland Clinic.
Pelin Batur, MD, Staff in the Department of Subspecialty Care for Women's Health, says leaders want women to feel heard, seen and supported.
The impetus came from the increasing demand by women, who have long experienced a dearth of answers to the kinds of health issues they face around menopause. In addition to menopause symptoms, this includes a host of other concerns, such as cognitive health, headaches, weight management, sleep disturbances, and breast and bone health.
“Historically, there has not been a lot of menopause education as part of endocrinology, primary care or gynecology training” says Dr. Batur. So if a physician didn’t have a natural interest in women’s midlife issues, they may not have felt as comfortable addressing them.
“Women used to be told, ‘Just stick it out. Your mom went through this fine, you'll get through it,’” says Dr. Batur. “Then we used to tell people, ‘Symptoms typically resolve by five years.’ Well, it turns out that symptoms last, on average, at least seven years. And for individuals of color, it’s more like a decade. A notable percentage of the population have symptoms for the rest of their life.
“Over the last 20 years, as awareness of the safety of treatments for menopause has changed, patients started demanding change,” she adds. “They were saying, ‘I don't feel I should suffer. Somebody should be able to hear me.’”
Advertisement
Results and interpretations of a landmark menopausal hormone therapy (MHT) trial by the Women’s Health Initiative (WHI), begun in 1998, set off alarm bells. The first results, published in 2002, indicated that participants who received estrogen/progestin combination therapy had an increased incidence of heart disease and breast cancer, as well as a reduction of colorectal cancer and osteoporotic fractures. That part of the trial was discontinued, generating alarm among clinicians and patients. Two years later, results for an estrogen-only study cohort showed a more favorable safety profile, but fears surrounding MHT persisted.
Before the trial, one in every five U.S. women over 40 was using MHT; after publication, nearly 90% of women discontinued their hormones.
Over the years, more nuanced research and analysis showed that — with careful attention to the time when MHT is initiated and the type of formulation used — the benefits of MHT for most women outweigh the risks. But that didn’t always quell clinicians’ concerns about prescribing MHT, even as their patients expressed the need for help with symptoms.
“In some cases, clinicians saw that the hormones can be safely administered, but they didn't feel they had enough training in them,” says Dr. Batur. “And then patients came saying, ‘I don't feel well and I need this addressed.’ So that has been driving change. The patient voice is driving a lot of the change.”
What distinguishes Cleveland Clinic’s Women’s Comprehensive Health and Research Center is a commitment to answering that call for care by reducing logistical and educational barriers and bridging knowledge gaps.
Advertisement
The patient access pillar of the initiative begins with the Welcome Center, a team of experienced and compassionate health navigators that patients can call to coordinate their care.
“These are some of our best and brightest navigators who really know the system well,” says Dr. Batur. “They spend up to 45 minutes on the phone with the patient to understand their needs, and then set them up for the correct services accordingly. I'm their clinical backup. If they're unsure of where a patient should receive the right care, they reach out to me.”
Patients might be offered a shared medical appointment aimed at helping them to understand the array of symptoms that can happen at midlife, as well as all of their holistic and prescription treatment options — all in the setting of a supportive group environment.
“If they're not interested in a group visit, then they can be seen one-on-one with the menopause specialist, typically within a few weeks” says Dr. Batur. “A lot of people like the group aspect because they learn from each other's questions. There's quite a bit of camaraderie in it. And they get 90 minutes of education about all their treatment options during this phase of life.”
Improving connections among specialists plays an important role in answering patient need.
“There are so many conditions that bridge specialty lines,” says Dr. Batur. “For example, take hormonal headaches. Neurologists know headaches, but they don't get a lot of training in hormones. OB/GYNs and endocrinologists know hormones, but they don't get a lot of training in headaches. Primary care has to address so many other things. Some diseases really don't have a medical home, but by creating connectivity, we work together to produce novel solutions for patients.”
Advertisement
The Women’s Comprehensive Health and Research Center also is creating a registry so individuals can be followed over time and be connected, if they wish, with research opportunities. “This will help us continue to break down subspecialty silos in research so that we can better understand these conditions,” Dr. Batur says.
For example, individuals who experience brain fog as part of the menopause complex can be seen by a neurology menopause team for further cognitive testing and education.
“We now have an ability to not only get patients to the right clinical service, but also offer them the opportunity to be in a research study where they can be followed over time,” Dr. Batur says.
The initiative provides physician support in an era when time is short and workloads have increased, making it difficult to find answers to more complex questions.
“It’s not as if doctors are not taking good care of patients,” says Dr. Batur. “We understand how complicated this is. We also understand how time-consuming many of these conversations and evaluations are. But women are really suffering. So we're trying to create innovative solutions to support your practices. We're happy to do some of the counseling and then refer patients back to their usual care team. We want to work with clinicians so that we help both patients and our colleagues.”
Patients can contact 216.444.8686 to speak with one of the patient navigators during typical business hours. The team strives to answer quickly and minimize hold times. Patients also can chat virtually with a health navigator via on the website. However, patients are strongly encouraged to call when they have time for a more comprehensive discussion of their needs.
Advertisement
Advertisement

Alzheimer’s studies delve into sex-related variances in the expression of the disease

Approximately 500 million people globally are experiencing 'period poverty'

Pediatric and adolescent reproductive providers are uniquely positioned to intervene

Findings reinforce the importance of multidisciplinary care

Plasma proteome analysis aimed at identifying candidate blood-based biomarkers in women
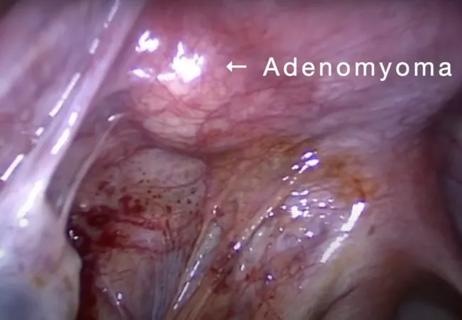
Laparoscopic surgery provides relief for teenage patient with adenomyoma and endometriosis

Multi-site study reveals surprising findings

Nutrition and cooking program supports maternal-infant health