Locations:

Better outcomes may be achieved through staged reconstruction
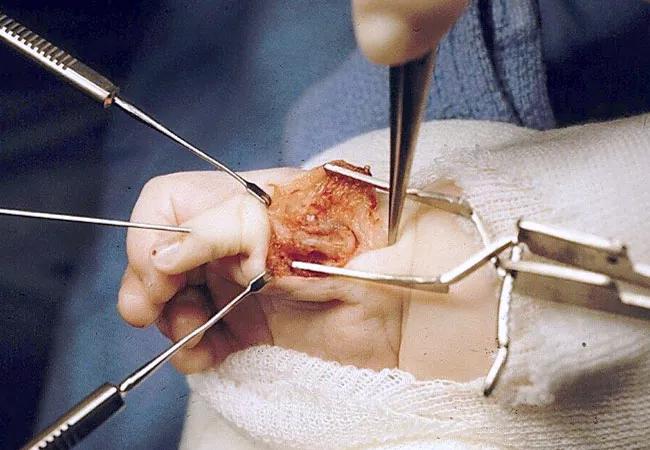
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9ebb84a5-bdfd-4ee7-aee9-ce6e334e8b27/19-ORT-1068-seitzBbyHandPhalanges-650x450_jpg)
19-ORT-1068-seitzBbyHandPhalanges-650×450
Congenital hand differences, as a group that includes syndactyly, thumb hypoplasia and cleft hand, are present in approximately 2 in every 1,000 live births. Thumb hypoplasia is very rare, and occurs only in 1 in every 100,000 births. There is a great deal of variation within thumb hypoplasia, which is defined as a short, underdeveloped or absent thumb. By applying the most recent developments in the field, such as opponensplasty, polliciztion, nonvascularized toe phalangeal transfer and distraction lengthening, we are able to restore function and maintain sensation in these young hands.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
At the outset of treatment, it is vital to set realistic goals for families through counseling and education. Generally speaking, the goal of thumb reconstruction is to provide a stable pedestal for prehension, as well as tactile sensation. Function of the hand is more important than cosmetic outcome, but increased function and dexterity translate directly into enhanced aesthetic use of the hand.
In more significant cases of hypoplasia, in which the carpometacarpal joint is absent and there is a poor skin bridge between the rudimentary thumb and the hand, a pollicization procedure may provide a functioning thumb. In pollicization, any existing thumb nubbin is amputated and another digit—generally the index finger—is repositioned to function as a thumb.
In some cases, pollicization may not be the only or best option. Parents sometimes hesitate with pollicization, as they may struggle to understand why “nubbin” amputation and replacement with the index finger may be necessary. Nonvascularized toe phalangeal transfer can provide functionally enhanced mechanical and prehension outcomes. In cases in which there is a shortened thumb or multiple digit involvement, nonvascularized toe phalangeal transfer may be indicated.
Roughly a decade ago, a patient with Blauth IIIB difference presented to our practice for a second opinion. His parents had been told that pollicization was the only reconstruction available, and we believed he was a good candidate for nonvascularized toe phalangeal transfer with staged reconstruction.
Advertisement
Under general anesthesia, we removed the second proximal toe phalanx from both feet, which were then inserted into the soft tissue beds we created below the remnant metacarpal. We secured the toe phalanx with a K-wire. We did not need to perform distraction lengthening because the transferred toe continued to grow.
After approximately six months, the toe bone had revascularized and was ready for the next stage of reconstruction, which included muscle and tendon transfers.
Following a period of progressive growth, we performed Huber opponensplasty and transfer of extensor indicis proprius to replace extensor pollicus longus function and flexor digitorum superficialis to replace flexor pollicis function.
In other cases, if growth is not adequate, additional functional length can be obtained through distraction lengthening, in which pins are inserted and the bone carefully divided and attached to an external frame, which can provide gradual lengthening. Following a five-day period of healing, the distraction lengthening process is begun, including four separate 0.25mm lengthenings each day.
This slow lengthening stretches out the fracture callus, and neo-osteogenesis is achieved through the stretched fracture callus. After a period of consolidation, the equipment is then removed and similar oppoentsplasty and tendon transfers are performed.
Generally, distraction lengthening generates little pain. Possible complications include premature consolidation, the development of angular deformities, skin breakdown, device failure, infection or soft-tissue injury, but close monitoring through regular follow-up visits minimize problems and complications.
Advertisement
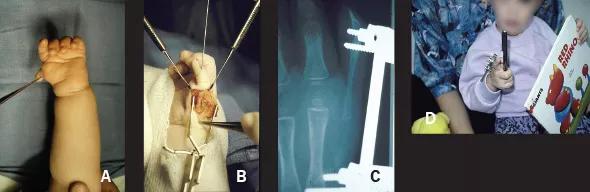
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/fc9d8a3d-3a0a-44b9-9ece-19591761cf18/Seitz-Thumb-Figure-1-Inset-590pxl-width_jpg)
A. Pre-operative photograph of six-month-old child’s hand with Blauth IIIB hypoplasia. B. Intraoperative photograph showing transferred toe phalanges. C. X-ray of distraction lengthening device, lengthening the transplanted bones to satisfactory length and alignment. D. Child is able to manipulate objects throughout distraction lengthening.At the 10-year follow up, the patient and his parents were pleased with the growth and functional status of the thumb.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c232c4d7-ad14-4731-a6d7-5e14fd9b5f7e/image-3-1_png)
X-ray image from 10-year follow-up.
Hands function as tactile antennae in developing children, and are used to explore their emerging universe. As a result, timing surgery so that patients can naturally explore and manipulate their surroundings is important for their overall development. Ideally, surgical intervention begins when the child is six months of age, before cortical patterning (i.e., the representation of the hand on the brain), and is complete before the child begins formal schooling. Thumb reconstruction early in life should restore a child’s ability to explore, improve the potential for bi-manual manipulation and allow for more normal cortical patterning.
Advertisement
Advertisement

Innovative procedure offers less-invasive alternative to Latarjet procedure

Even patients with reported penicillin allergies can receive it without increased complications

Study challenges assumptions about risk evaluation in total hip revision

Protein expression in synovial fluid indicates patients’ immune factors may be involved

Cleveland Clinic’s Global Peak Performance Center and PGA TOUR partnership pair advanced assessment with longitudinal follow-up to enhance clinical decision-making

Study highlights the need for objective functional measures as value-based care expands

Reduces likelihood of achieving CMS-defined substantial clinical benefit at one year

Step counts suggest recovery is more variable and individualized than commonly believed