Locations:

Procedure offers potential for less pain and faster recovery in selected patients
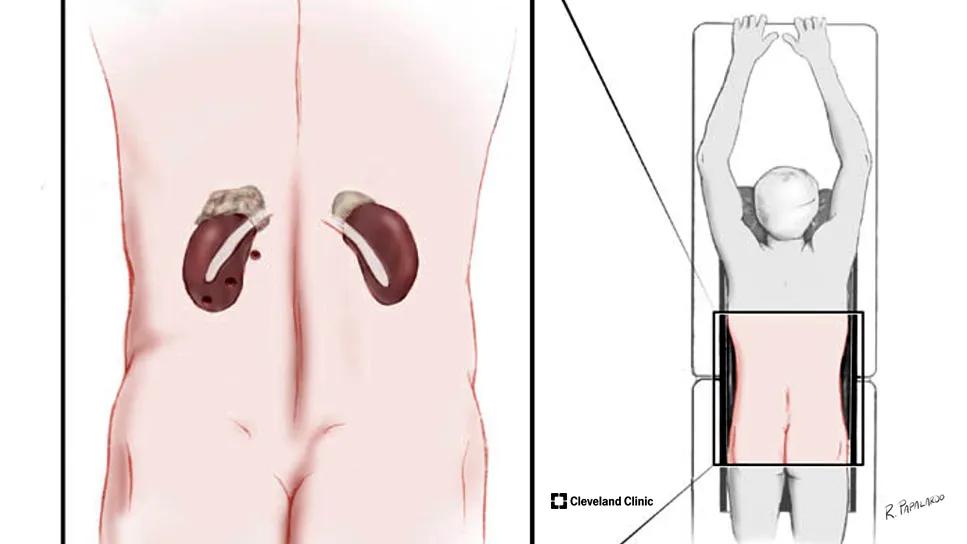
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4cf57988-c0f6-4ebe-b808-d27f31f3d060/medical-illustration-posterior-adrenalectomy-hero)
Medical diagram of adrenal glands seen through the back of a patient
For high-volume adrenal surgery centers, such as Cleveland Clinic’s Adrenal and Neuroendocrine Tumor Center, it’s important to be able to offer surgical options geared toward individual patients and adrenal tumor characteristics, thereby optimizing outcomes.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Each year, Cleveland Clinic performs nearly 150 adrenal surgeries using the mini posterior retroperitoneal approach, lateral transabdominal approach, robotics and adrenal ablation.
Consult QD recently talked with Eren Berber, MD, about the endoscopic posterior retroperitoneal adrenalectomy, also called the mini “back scope adrenalectomy” (MBSA), which can be performed laparoscopically and robotically. Dr. Berber is Director of Robotic Endocrine Surgery and the Adrenal and Neuroendocrine Tumor Center.
What are the advantages of mini back scope adrenalectomies compared to the lateral transabdominal approach?
MBSAs are used to remove adrenal tumors through three small incisions – ranging between five and 10 millimeters – through the back of the patient. This posterior approach provides a more direct and faster exposure of the adrenal gland, avoiding the abdominal cavity, so patients may experience less pain and faster recovery.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c2e20be9-4c80-4fe5-9c79-a254d22d353f/medical-illustration-posterior-adrenalectomy-inset)
What patients make the best candidates for MBSA?
You must select patients very carefully. When you perform posterior surgery, the surgical space is smaller. In general, candidates for this procedure are patients with:
Patients who have previously had extensive abdominal surgeries and scarring are often ideal candidates for mini back scope adrenalectomy because minimally invasive options through the front or the side may not be possible or easy. Going through the back avoids scarring, so it’s a very efficient alternative.
Advertisement
In addition, patients with bilateral tumors are good candidates. If you perform the adrenalectomy through the side (lateral transabdominal approach), you must change the position of the patient in between gland removals. If you use the posterior approach, you don’t have to switch positions.
Are there specific factors that contribute to the success of the procedure?
Multidisciplinary preoperative assessments of patients with adrenal tumors are critical. In our program, these patients undergo a comprehensive hormonal evaluation in collaboration with endocrinologists. We also team up with dedicated adrenal radiologists to assess any lesions for malignancies using sophisticated imaging techniques. Finally, experience of the surgeon is important.
Can you delve a bit more into the advanced imaging and hormonal evaluations?
Sure. So, we first do a non-contrast CT of the adrenal glands which allow us to measure the fat content. And if the fat content is high, those lesions are going to be benign. When the fat content is low, we conduct an additional assessment by giving the patient a contrast agent and measuring how fast it is cleared by the tumor. If the contrast is cleared fast, then it's most likely a benign tumor. But if the contrast is not cleared fast, then there is a risk of malignancy in that tumor.
You can also perform an MRI to gather the same information. At our center, we use both imaging modalities to make this assessment. We also have a multidisciplinary tumor board that meets with representatives from various specialties to discuss challenging cases to reach a consensus decision.
Advertisement
We’re also seeing an increased number of patients with mild autonomous cortisol secretion, or MACS, which causes metabolic complications such as high risk for hypertension, diabetes, osteoporosis and cardiovascular events, such as arrhythmias and coronary artery disease. Diagnosis of this condition requires dexamethasone suppression testing and demonstration of low adrenocorticotropic hormone levels.
We make a concerted effort to ensure that the patient has a comprehensive hormonal evaluation preoperatively to help achieve the best outcomes.
Is MBSA a more challenging procedure for surgeons compared to other adrenalectomy approaches?
In general, surgeons are more familiar with intra-abdominal anatomy, and therefore the learning curve for the posterior approach is steeper than the lateral transabdominal approach. However, with good mentoring and proctoring, this procedure can be mastered.
Cleveland Clinic was one of the first centers in the U.S. to incorporate MBSA into the treatment of adrenal tumors beginning in 2000. And in 2009, we became the first center to describe the robotic posterior adrenalectomy procedure in the world.
Since then, we have been offering adrenalectomies through both an MBSA and lateral transabdominal approaches. Having a high-volume adrenal program is important as studies have shown that patient outcomes are improved in high-volume centers and being experienced in different approaches allow us to create a custom surgical plan for every patient. This is critical for a good patient experience. For instance, the MBSA approach might be best for a patient with a small tumor away from critical structures in the absence of abundant amount of fat around the adrenal and kidney, while a lateral transabdominal approach might be best for a patient with a large tumor close to critical structures in the presence of abundant amount of fat around the adrenal gland.
Advertisement
Advertisement

Challenges include multimorbidity, polypharmacy, limited mobility and sarcopenia

Data could help inform policy and patient-provider conversations

Pheochromocytoma case underscores the value in considering atypical presentations

Advocacy group underscores need for multidisciplinary expertise

A reconcilable divorce

A review of the latest evidence about purported side effects

High-volume surgery center can make a difference

Advancements in equipment and technology drive the use of HCL therapy for pregnant women with T1D