Locations:

Innovative approach to living-tissue AVR achieves low reintervention rates, excellent long-term survival
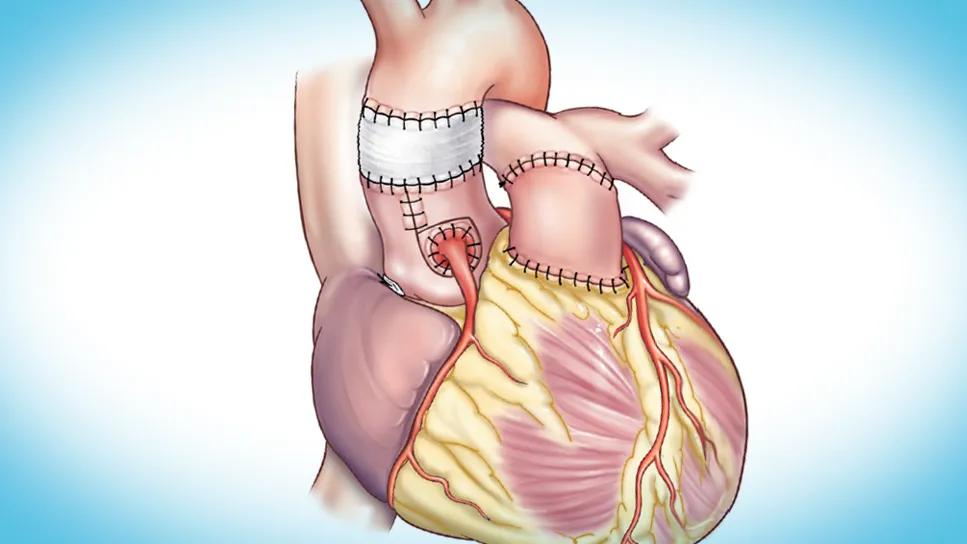
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e025ac4d-7290-4fa7-88cc-899b3a37b982/cqd-ross-procedure-hero)
illustrated human heart with several sutured parts
Progressive dilation is a common cause of autograft failure after the Ross procedure for aortic valve replacement. Cleveland Clinic surgeons have found success in mitigating this dilation with a “semi-inclusion” modification they developed to provide native tissue autograft support.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
According to results presented at the 2026 annual meeting of the American Association for Thoracic Surgery (AATS), the technique improves operative and clinical outcomes, which the surgeons attribute to enhanced exposure of the aortic annulus, simplification of coronary button implantation and preservation of the physiologic motion of the aortic root. Specifically, a review of 58 cases from 2000 to 2021 demonstrated no mortalities to date and 100% freedom from reoperation on the autograft at 10-year follow-up.
“Our semi-inclusion technique offers a reproducible method for wrapping the autograft in native tissue rather than synthetic graft material,” says Cleveland Clinic cardiothoracic surgeon Shinya Unai, MD. “This approach mitigates progressive dilation while preserving the dynamic motion of the root during the cardiac cycle.”
He explains that wrapping the autograft in synthetic grafts, although technically simpler, restricts this motion and may alter valve geometry over time, potentially leading to failure. “The semi-inclusion technique, which was pioneered by Cleveland Clinic surgeon Gosta Pettersson, MD, PhD, was developed to preserve native tissue and minimize foreign material using a simplified wrapping process,” Dr. Unai notes.
The procedure begins with deconstruction of the aortic root through creation of symmetric flaps of tissue around the coronary buttons, preserving the non-coronary sinus and the left-right commissure with wings for later reattachment (panel A in figure below). A running suture annuloplasty is performed to stabilize or downsize the annulus if needed.
Advertisement
The autograft is then prepared and implanted with a running suture (panel B), followed by reimplantation of the coronary buttons. Reconstruction of the native root involves tacking the midpoint of the pulmonary commissures to the surrounding native tissue and passing the wings of the coronary sinuses over the buttons, suturing them to the adjacent non-coronary sinus tissue. This encloses the autograft within native aortic tissue (panel C). Next, an interposition graft is sewn to the distal autograft, incorporating native tissue to stabilize the sinotubular junction (panel D). Key steps in the technique are illustrated below.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/321f8fbc-fbcd-4f90-8d40-3f74f020c4bf/cqd-ross-procedure-inset)
Key steps in the semi-inclusion Ross modification technique. The steps shown in panels A through D are detailed in the two paragraphs above. Panel E shows the completed modified Ross procedure. LCA = left coronary artery; RCA = right coronary artery.
“This technique improves exposure of the aortic annulus and the subvalvular apparatus by splaying open the root before autograft implantation,” Dr. Unai explains. “It permits a more traditional coronary button implantation, avoiding the kinking risk associated with passing buttons through two tissue layers, which is what’s done in other native inclusion methods.”
He adds that this approach also allows a tailored fit of native tissue around the autograft, enabling modification of the reconstructed aorta through plication or augmentation using additional ascending aorta tissue.
The recent AATS presentation shared results from a retrospective review of all 58 patients who underwent a Ross procedure with the semi-inclusion technique at Cleveland Clinic from 2000 to 2021. Among this sample, 56% had a bicuspid aortic valve, the mean aortic root diameter was 3.2 cm and 36% of patients had a previous sternotomy. More than half of patients (55%) had mixed aortic stenosis and aortic regurgitation.
Advertisement
Among the findings:
“From a cardiology perspective, these results are particularly compelling because they demonstrate preservation of excellent valve hemodynamics over the long term, with stable gradients and minimal aortic regurgitation,” notes Serge Harb, MD, staff cardiologist in Cleveland Clinic’s Section of Cardiovascular Imaging. “The Ross procedure is certainly an attractive option, particularly for younger patients requiring aortic valve replacement, and these data suggest that thoughtful technical refinements such as the semi-inclusion technique can further enhance its durability. The combination of outstanding hemodynamic performance, 100% survival and freedom from autograft reoperation at 10 years is impressive.”
“By enhancing aortic annulus exposure and simplifying coronary button implantation, our semi-inclusion modification of the Ross procedure may help promote broader adoption of living-tissue aortic valve replacement in appropriate patients,” Dr. Unai concludes.
Advertisement
Advertisement

‘Sac flow’ is more precise and will ease unfounded patient concerns, experts argue

Expert advice on repair vs. replacement, timing of surgery in asymptomatic cases and much more

Modified-Bentall single-patch Konno enlargement (BeSPoKE) optimizes hemodynamics, facilitates future TAVR

Experience-based takes on valve-sparing root replacement from two expert surgeons

30-year study of Cleveland Clinic experience shows clear improvement from year 2000 onward

Surgeons credit good outcomes to experience with complex cases and team approach

For many patients, repair is feasible, durable and preferred over replacement

In experienced hands, up to 95% of patients can be free of reoperation at 15 years