Locations:

Modified-Bentall single-patch Konno enlargement (BeSPoKE) optimizes hemodynamics, facilitates future TAVR
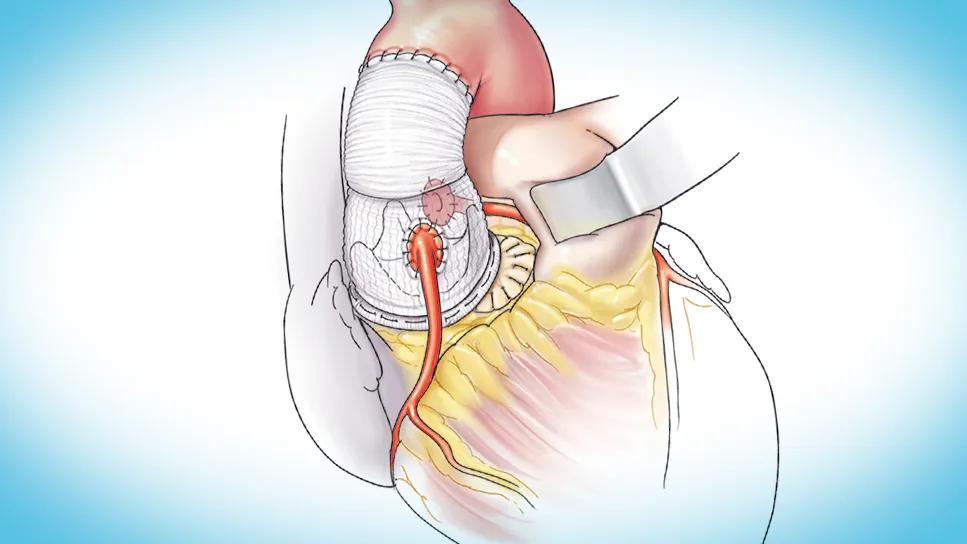
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3fbf9ecb-a53c-411c-9917-ed53e1fecb07/BeSPoKE-technique-cqd-feature)
illustration of human heart with a graft repair
For adults facing complex left ventricular outflow tract (LVOT) obstruction coupled with severe aortic stenosis or persistent prosthesis-patient mismatch (PPM), a novel surgical strategy offers significant hemodynamic improvements and establishes favorable anatomy for future transcatheter aortic valve replacement (TAVR).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The approach, developed at Cleveland Clinic, is called the modified-Bentall single-patch Konno enlargement (BeSPoKE) technique. Its developers recently described it in an article featured on the cover of the Annals of Thoracic Surgery (2025;120[1]:51-61), which also reported results in a series of 25 patients.
The technique safely addresses small aortic annuli and subvalvular obstruction, the paper reports, allowing for consistent placement of larger aortic prostheses and dramatically reducing transprosthetic gradients. “We have shown that BeSPoKE is an effective treatment strategy,” says lead author Eric Roselli, MD, Cardiac Surgery Director of Cleveland Clinic’s Aorta Center, “particularly for patients with severe prosthesis mismatch or an aortic annulus smaller than 21 mm who require reintervention or initial aortic valve replacement.”
Surgical management of LVOT obstruction and PPM in adults is notoriously challenging, and decision-making about the need for aortic annular or root enlargement remains a topic of debate. PPM is an enduring problem, complicating surgery for individuals with small LVOTs, and it leads to early structural valve failure and progressive left ventricular hypertrophy.
Established posterior enlargement procedures — such as the Nicks and Manouguian techniques, and even the more recent Y technique — extend to or into the annulus, but they often depend on supra-annular replacement to fit larger prostheses and may not sufficiently address subvalvular obstruction at the level of the mitral valve. Approaches focused solely on hypertrophic cardiomyopathy, such as septal myectomy, address subannular obstruction but fail to solve the small annulus problem. Notably, the primary survival benefit of surgical repair of LVOT obstruction can be attributed to enlarging the indexed effective orifice area, and this requires addressing narrowing at both the subvalvular and valvular levels.
Advertisement
The landscape has grown more complex with the rise of TAVR. While TAVR expands treatment options for high-risk patients, it complicates later surgical intervention when TAVR fails or the patient is deemed ineligible for TAVR due to anatomic issues like low coronary arteries. For instance, almost one-third of patients in the BeSPoKE study cohort were referred after being excluded from valve-in-valve TAVR because of anticipated obstruction of low-lying coronary arteries or incompatibility of their current prostheses due to small size.
“Drawing insights from the pediatric cardiac surgery experience with the Konno procedure,” Dr. Roselli explains, “we developed the BeSPoKE technique to reproducibly and reliably enlarge both the aortic annulus and the LVOT with a simplified single-patch technique for adults presenting with this complicated combination of valve and subvalvular disease.”
The BeSPoKE procedure integrates three critical therapeutic goals in a single operation:
The technique facilitates root enlargement via an anterior septoventriculoplasty within the outflow tract. This involves performing an anterior ventriculoseptotomy, extending downward into the left ventricle. The resulting defect is reconstructed using a single pericardial patch that extends from within the left ventricular portion of the septal defect into the medial portion of the right ventricular outflow tract. This patch defines a new, larger aortic annulus (neoannulus). This is followed by a composite valve-graft root replacement (Bentall style), securing the composite graft across both the native annulus between the trigones and the anterior patch portion of the newly defined neoannulus. This modified approach simplifies the root implant by using a single patch for the reconstruction.
Advertisement
By resecting obstructive outflow tract lesions and completing a true anterior enlargement, the technique optimizes ventricular function and facilitates placement of a large prosthesis. “The composite root replacement ensures the coronary arteries are reimplanted well above the sewing ring of the valve, thereby increasing coronary height,” Dr. Roselli observes. “This helps overcome common anatomic exclusions to future transcatheter interventions, if needed.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cc00d8e3-3713-4b97-9335-f0ba4d641a39/BeSPoKE-technique)
Key steps of the BeSPoKE technique, from anterior annular enlargement using septotomy (A) to septal myectomy and exposure of the right ventricular outflow tract (B) to single-patch septoventriculoplasty (C) to composite valve-graft Bentall-style root replacement. The completed procedure is shown in panel E. Reprinted from Roselli et al., Annals of Thoracic Surgery (2025;120[1]:51-61). © 2024 Cleveland Clinic Foundation.
The authors’ Annals of Thoracic Surgery report shares outcomes for 25 consecutive adults who underwent the BeSPoKE procedure at Cleveland Clinic between October 2017 and March 2022. Median age was 60 years, and 84% were women. The cohort was clinically complex: 84% had prior AVR, generally with a small implant size (median of 19 mm), and subsequently developed severe aortic stenosis combined with PPM (mean indexed effective orifice area of 0.41 ± 0.15 cm2/m2). Median follow-up was 2.1 years.
The study demonstrated consistent success in achieving therapeutic goals:
Advertisement
Overall survival was excellent, with no operative deaths (in-hospital or within 30 days). Survival remained high at one year (96%) and two years (92%). No reoperations for aortic valve issues or structural valve failure were reported during the median 2.1-year follow-up.
However, the technical complexity and aggressive nature of the anterior septoventriculoplasty are associated with notable electrophysiologic risk. Postoperative complications included atrial fibrillation in 36% of patients and complete heart block requiring permanent pacemaker placement in 32%.
“While the risk of needing a permanent pacemaker was high, it is likely worth the significant hemodynamic benefit achieved by BeSPoKE, especially considering the severe consequences of poor valvular hemodynamics,” Dr. Roselli says.
“Dealing with a very small annulus and LVOT obstruction requires anterior interruption of the annulus, as depicted with the BeSPoKE technique,” says Hani Najm, MD, MSc, Chair of Pediatric and Congenital Heart Surgery at Cleveland Clinic, who was not involved in the study. “This technique also aligns the ventricular septum with the aorta, creating an unobstructed outflow tract.”
The investigators conclude that their study confirms that BeSPoKE improves both anatomic and physiologic conditions by enabling prosthesis upsizing and significantly improving hemodynamics, all while making transcatheter reintervention a viable future option. Despite the strong short-term outcomes, they note, longer follow-up is needed to assess repair durability and future valve-in-valve TAVR outcomes.
Advertisement
“The BeSPoKE technique represents an important strategy for managing severe LVOT obstruction and prosthesis mismatch in adults,” Dr. Roselli observes. “Successful execution relies heavily on deliberate anatomic dissection to minimize injury to the conduction system as well as the expertise of a high-volume aorta center.”
Advertisement

‘Sac flow’ is more precise and will ease unfounded patient concerns, experts argue

Innovative approach to living-tissue AVR achieves low reintervention rates, excellent long-term survival

Expert advice on repair vs. replacement, timing of surgery in asymptomatic cases and much more

Experience-based takes on valve-sparing root replacement from two expert surgeons

30-year study of Cleveland Clinic experience shows clear improvement from year 2000 onward

Surgeons credit good outcomes to experience with complex cases and team approach

For many patients, repair is feasible, durable and preferred over replacement

In experienced hands, up to 95% of patients can be free of reoperation at 15 years