Locations:

Focused ultrasound is paired with ALA to utilize sonodynamic therapy to target cancer cells

Cleveland Clinic is the first institution to open enrollment for a new multicenter study to identify the optimal drug and energy dose schedule for a new combination therapy to treat recurrent glioblastoma (GBM). The novel therapy is designed to deliver a one-two punch to the disease utilizing sonodynamic therapy (SDT) to directly target GBM cells and leave normal brain cells unharmed.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
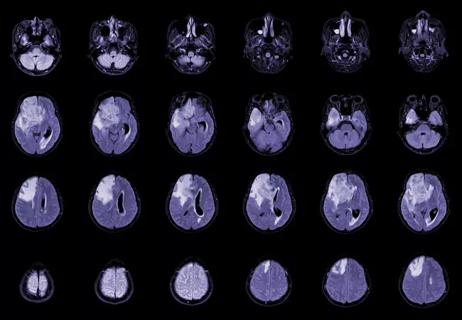
GBM, the most common malignant primary brain tumor in adults, is nearly universally fatal. “There is very little we can do to slow the disease process,” says Matthew Grabowski, MD, a neurosurgeon with Cleveland Clinic’s Rose Ella Burkhardt Brain Tumor and Neuro-Oncology Center who serves as site principal investigator for the study. “This state-of-the-art therapy is noninvasive and has the potential to halt progression of these tumors.”
SDT involves the use of MRI-guided focused ultrasound (MRgFUS) to activate the drug SONALA-001 (aminolevulinic acid [ALA]), a small-molecule prodrug of protoporphyrin IX (PpIX) that is preferentially absorbed by tumor cells. MRgFUS is a noninvasive, low-frequency form of focused ultrasound.
In preclinical studies, performing SDT with MRgFUS and SONALA-001 has been shown to slow growth of gliomas and greatly extend survival in animal models of the disease. A first-in-human phase 0 trial found that SDT with ALA (i.e., ALA SDT) was well tolerated, was not associated with off-target cellular or radiographic effects, and provided direct evidence of reactive oxygen species formation and targeted tumor cell death in recurrent GBM.
The new research is an open-label phase 1/2 study (NCT05370508) of SONALA-001 in combination with Exablate 4000 Type-2 MRgFUS. Phase 1 involves testing various drug and FUS energy dose combinations of ALA SDT — specifically, 10 mg/kg and 20 mg/kg of SONALA-001 and 200J, 400J and 800J of FUS energy — to determine the recommended dose for phase 2 testing. The study will then assess two and three ALA SDT treatments, each separated by a 28-day cycle, to define the recommended treatment schedule for phase 2 testing.
Advertisement
Once the dose and schedule are established, approximately 30 additional patients will be enrolled in phase 2 testing, which will assess the safety and efficacy of ALA SDT at the optimized drug/energy dose combination and treatment schedule.
Cleveland Clinic is participating in both phases of testing. Twenty-seven patients will be enrolled across eight study sites for phase 1 and the approximately 30 patients in phase 2 will be enrolled across 15 sites.
Safety assessments include the frequency and severity of adverse events/adverse device effects (AEs/ADEs), serious AEs/ADEs and dose-limiting toxicities, as well as laboratory testing, vital signs, electrocardiographic assessment, and neurologic and physical examinations.
MRI will be used at treatment cycles 2 to 5, cycle 7 and every three cycles thereafter until documented disease progression. Efficacy is evaluated in terms of objective response rate per modified response assessment in neuro-oncology (mRANO), clinical benefit rate, duration of response and clinical benefit, time to response, and progression-free survival at 6 and 12 months. Overall survival from treatment initiation until death from any cause will be assessed.
MR perfusion will be performed with dynamic contrast-enhanced MRI and dynamic susceptibility contrast MRI to evaluate changes in vessel density and vascularity that may reflect response to ALA SDT. Diffusion-weighted imaging and diffusion tensor imaging will be obtained to evaluate for changes in cell density and extracellular water that may reflect tumor response. T1 maps and susceptibility-weighted imaging will be acquired immediately before and after MRgFUS application to detect regional changes in oxidative stress and free radical formation.
Advertisement
Adults with primary (de novo) GBM at first or second recurrence/progression for whom resection is not indicated are eligible to participate in the study. Tumors must be supratentorial, contrast-enhancing and bidimensionally measurable with a volume of 5 to 30 mL, based on MRI within 14 days prior to study initiation.
“Many glioblastoma trials exclude patients who have had certain previous treatments or are at their second recurrence, but that is not the case with our study,” Dr. Grabowski notes. “Tumors in the brainstem or cerebellum are excluded because this technology is best suited for more superior and centrally located lesions.”
Previously tested at Cleveland Clinic for treatment of Parkinson disease and other movement disorders, the Exablate 4000 is an ultrasound transducer worn like a helmet. The piezoceramic device can be adjusted to a patient’s skull and delivers ultrasound at a frequency of 650 KHz. “We’re one of the few institutions with significant experience using both the Type 1 and Type 2 Exablate systems,” Dr. Grabowski says, adding that the treatment takes about one to three hours.
“If this protocol works, it could be a tremendous benefit because there is currently no well-defined, targeted standard of care in recurrent glioblastoma,” he concludes. “Our hope is to extend survival and improve quality of life in individuals with this devastating disease.”
Advertisement
Advertisement

Phase 2 trials investigate sitagliptin and methimazole as adjuvant therapies

Advances in genomics, spinal fluid analysis, wearable-based patient monitoring and more

Researchers use AI tools to compare clinical events with continuous patient monitoring

Combining dual inhibition with anti-PD1 therapy yielded >60% rate of complete tumor regression

Cleveland Clinic researchers pursue answers on basic science and clinical fronts
New research from Cleveland Clinic helps explain why these tumors are so refractory to treatment, and suggests new therapeutic avenues

Presurgical planning and careful consideration of pathology are key to achieving benefits
Study demonstrates its role in tumor lethality, raises prospect of therapeutic targets