Locations:

Conservative approach a good option for some TMD patients

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1a8a12fe-d599-4162-acfa-03b48e09415e/HNI_2740973_02-24-22_045_AMO-jpg)
Tooth model
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The comprehensive treatment of temporomandibular disorders (TMDs) is one focus of the Head & Neck Institute/Section of Dentistry and Oral and Maxillofacial Surgery. Conservative primary management of TMDs and associated pain typically includes splint therapy, patient education and adjunctive therapies through referral for physical therapy, pain management and cognitive behavioral therapy.
Yet even when these interventions successfully correct TMD symptoms, some patients are left with an anterior open bite secondary to condylar changes and repositioning of the condyles in the articular fossa. One approach to correcting such a malocclusion is orthodontics with orthognathic surgery. However, the prospect of facing surgery and the possible return of facial pain often lead patients to reject this interventional option.
The two brief case reports that follow describe a conservative alternative to surgery for correcting an anterior open bite. In both cases, the initial treatment had resulted in an acceptable level of comfort and confirmation of a stable temporomandibular joint (TMJ) position, but the patients were still left with an anterior open bite. To correct this problem, an orthodontist and an oral surgeon used temporary anchorage devices (TADs) in lieu of orthognathic surgery to treat the malocclusions. The outcomes of these patients suggest that this conservative approach is a promising option for selected patients who are reluctant to undergo orthognathic surgery.
TADs are temporary mini-implants used to provide anchorage to prevent tooth movement during orthodontic procedures. These minimally invasive small implants are placed in the maxilla or mandible between adjacent roots, and they are removed following the procedure. The implants provide the forces needed to intrude posterior teeth.
Advertisement
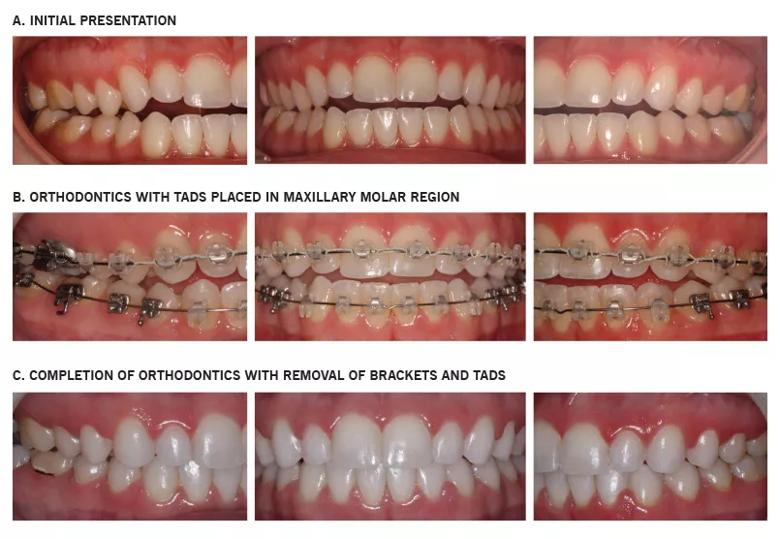
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/805d46be-6887-4fec-a328-da205adf74e1/16-ENT-2722-Kahn-Inset-Image-02-805pxl-width_jpg)
Case 1. A 28-year-old woman presented with a multiyear history of bilateral facial and TMJ pain, TMJ clicking, chronic headache, intermittent ear pain and neck pain. Her previous treatment included pain management, participation in Cleveland Clinic’s IMATCH program (Interdisciplinary Method for the Assessment and Treatment of Chronic Headache), physical therapy and dental orthotics (splints).
The use of a stabilization splint had eased her headaches and facial pain while the patient was under our care. She was referred for pain management, where she was treated with interarticular injections, pharmacotherapy and botulinum toxin A injections to the cervical and masticatory muscles. Her symptoms subsided to a manageable level, and with continued use of the splint, we were able to confirm that her occlusion remained stable.
While this initial treatment ameliorated the patient’s TMD symptoms, it left her with a malocclusion and an anterior open bite. Orthodontics with the use of TADs was completed in 2013 by a community orthodontist/oral surgeon (Figure). The patient was also given a dental night guard for retention and to prevent nocturnal bruxism. As of now, her occlusion remains stable.
Case 2. A 41-year-old woman came to us with an 18-month history of severe TMJ pain and dysfunction. Her TMD included anteriorly displaced TMJ disks without recapture. She also had a history of difficulty with eating and talking, as well as limited jaw opening. A dental splint had relieved most of her pain prior to her visit in our office, but she still complained of difficulty chewing because of a severe malocclusion and anterior open bite.
Advertisement
We initially managed the patient’s existing splint over a period of time, which allowed us to confirm that her TMJs were stable. Orthodontics was then recommended to correct her malocclusion. She consented to orthodontics but was not interested in orthognathic surgery. Therefore, TADs were placed by another local orthodontist/oral surgeon. The patient continues to undergo orthodontics.
For these two patients, orthodontics with the use of TADs provided a functional alternative to orthognathic surgery. This conservative approach may be preferable for patients disinclined to surgery and for those for whom conservative orthodontics is more accessible from a geographic standpoint.
Dr. Kahn is a general dentist in the Head and Neck Institute/Section of Dentistry and Oral and Maxillofacial Surgery and a Consultant for Craniofacial Pain and Jaw Dysfunction.
Advertisement
Advertisement

How effective management integrates multiple specialties and therapies

Systematic review indicates more can be done for higher-risk patients

Analysis of HNSCC patients shows HPV status to be predictive of higher abundance of oncobacteria within the tumor

Case study illustrates the potential of a dual-subspecialist approach

Evidence-based recommendations for balancing cancer control with quality of life

Study shows no negative impact for individuals with better contralateral ear performance

HNS device offers new solution for those struggling with CPAP

Patient with cerebral palsy undergoes life-saving tumor resection