Locations:

A new classification system proposed for common extensor tendinopathy

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/75ab5be4-34b9-4de1-a847-3329dbadb24a/20_HEN_1872897_Drago_04-10-20_YKL_36-jpg)
Tennis player
By Dominic King, DO, and Jason Genin, DO
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Terms like “tennis elbow,” “lateral epicondylitis” and “chronic elbow tendinitis” have historically been used interchangeably in research publications and by health care providers to describe nonruptured pathology of the common extensor tendon of the elbow. However, these terms do not always characterize or reflect the true underlying intratendinous pathology. Some patients clinically present with an acute “inflammatory” tendinopathy, some with a chronic “degenerative” tendinopathy and others as a mix of these presentations. While it is generally accepted that tendinopathy develops due to overloading of tensile and compressive forces of the tendon over time, the natural progression of tendinopathy is not well understood.
As with any disease entity, the ability to choose appropriate treatment relies on an accurate diagnosis. Today, therapies for common extensor tendinopathy are wide-ranging and include physical therapy, instrument-assisted manual therapy, counterforce bracing, corticosteroid injections and more recently, platelet rich plasma (PRP) injections, bone marrow and adipose-derived stem cell injections, placental-derived extracellular matrix injections and ultrasound-guided percutaneous tenotomy procedures.
Recent research that our team members were involved in has demonstrated that there is significant variability in the outcomes of common extensor tendinopathy therapies, specifically orthobiologics. Our hypothesis is that this treatment outcome variability exists because of the variability in tendon pathologies. While musculoskeletal ultrasound (MSK-US) has given us a reliable tool to outline different tendinopathy features, there has not been a widely-accepted classification system that has organized these findings.
Advertisement
To accurately compare the outcomes of tendon therapies, we first need to know that we are treating the same pathologic stage of tendinopathy. A reliable classification system for common extensor tendinopathy is a necessity.
MSK-US research on different pathologic features of common extensor tendinopathy has yielded these definitions:
We constructed a new classification system based on these MSK-US identified features, and organized them into four distinct pathologic types (Figure 1).
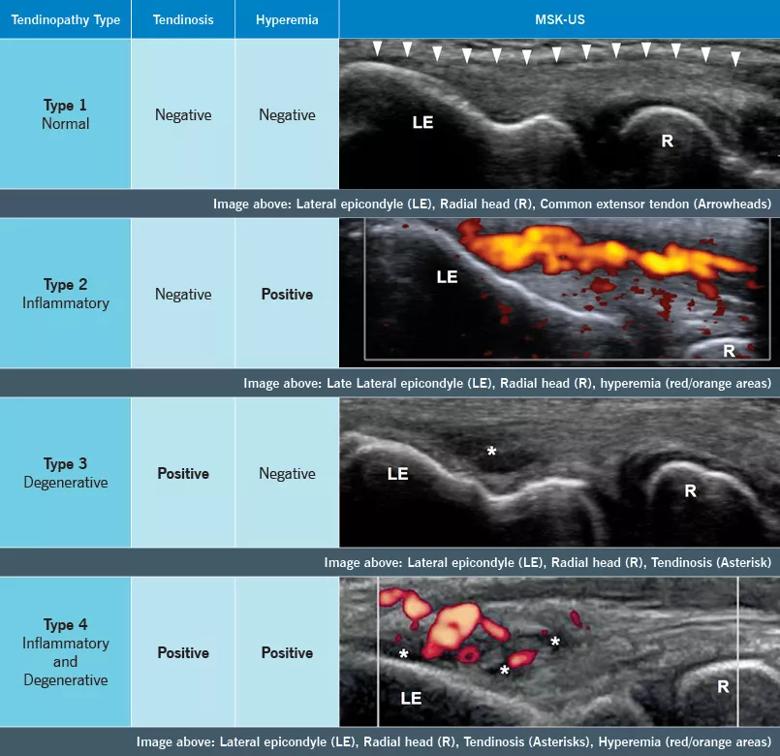
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/46399558-6f28-4086-a5b5-243bbfd96029/20-ORI-1961400-Updates-CQD-Graphic_jpg)
We have also worked with the OrthoMidas Episode of Care (OME) team in our department to develop an OME Tendinopathy Module for our electronic medical record. The module will feature this classification system for common extensor tendinopathies.
This integration will allow us to establish a prospective cohort and longitudinally track the outcomes of our office-based injections and procedures on these various grades of common extensor tendinopathy.
While this classification system may serve as a step toward more reliable and accurate tendinopathy research, rigorous reliability and prospective studies will ultimately determine its clinical usefulness to help guide tendinopathy treatment. If successful, this classification could be used as a research standard for all common extensor tendinopathy treatments, including physical rehabilitation and therapy, bracing, orthobiologic injections and any minimally invasive office-based common extensor tendinopathy procedure. We have a great deal of work ahead of us, and we welcome your candid feedback regarding this new classification system.
Advertisement
Chahla J, Cinque ME, Piuzzi NS, Mannava S, et al. A call for standardization in platelet-rich plasma preparation protocols and composition reporting: a systematic review of the clinical orthopaedic literature. J Bone Joint Surg Am. 2017 Oct 18;99(20):1769-1779.
Drs. King and Genin, sports medicine and medical orthopaedic physicians, are on staff in the Sports Health Center and Joint Preservation Center.
Advertisement
Advertisement

Innovative procedure offers less-invasive alternative to Latarjet procedure

Even patients with reported penicillin allergies can receive it without increased complications

Study challenges assumptions about risk evaluation in total hip revision

Protein expression in synovial fluid indicates patients’ immune factors may be involved

Cleveland Clinic’s Global Peak Performance Center and PGA TOUR partnership pair advanced assessment with longitudinal follow-up to enhance clinical decision-making

Study highlights the need for objective functional measures as value-based care expands

Reduces likelihood of achieving CMS-defined substantial clinical benefit at one year

Step counts suggest recovery is more variable and individualized than commonly believed