Locations:

A surge in transplants, advanced surgical techniques and multidisciplinary collaboration has helped shape and expand the Liver Transplant Program

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1a65a94a-3ae2-4c46-8c62-f5751d3c5494/CCC_Tadiello_3561108_Dr-Kwan-Liver-Transplant_01-23-23_MLC)
Dr. Kwan and Dr. Hashimoto performing Laparoscopic Liver Transplant Surgery
From the inception of Cleveland Clinic’s Liver Transplant Program in 1983, when the first transplant at Cleveland Clinic was performed, up until 2004, the number of annual liver transplants hovered around 30 patients. When Charles Miller, MD, joined Cleveland Clinic as Director of Liver Transplantation that year, the number of annual transplants increased to almost 100 cases per year. In 2025, that number increased to just under 300 transplants.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“I think there are several reasons for the growth of liver transplantation at Cleveland Clinic,” says Koji Hashimoto, MD, PhD, Director of Liver Transplantation at the Cleveland Clinic Main Campus and Professor of Surgery at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University. “We have done many kinds of transplants, and we have brought several innovations to the practice. Those include living donor transplant and minimally invasive living donor hepatectomy. We’ve also been able to take on higher-risk liver transplants, including combined cardiac surgery and liver transplants, and simultaneous multi-organ transplants. Machine perfusion has allowed us to preserve organs longer and reduce waiting times for patients. These developments have all had a cumulative effect on our ability to grow and expand our Liver Transplant Program.”
Recently, Cleveland Clinic’s Main Campus ranked No. 3 out of 143 U.S. liver transplant centers. Since 2012, the number of annual living donor transplants performed at Cleveland Clinic has also steadily increased.
“We expect to continue to see a rise in both deceased and living donor volume,” says Dr. Hashimoto. “However, increasing living donor volume is challenging because it’s not always easy or straightforward to find someone willing to donate part of their liver. Now, we have a new living donor liver transplant program director in Alejandro Pita, MD, FACS, and he has been working very hard to expand the program with the new living donor champion program to help transplant candidates find a living donor.”
Advertisement
Dr. Hashimoto believes that the increase in the Program’s volume is also due in part to the training and skills of the transplant surgeons and hepatologists at Cleveland Clinic. The vast experience of these surgeons, combined with the multidisciplinary collaboration at Cleveland Clinic, allows patients who may have been deemed too risky at other medical centers to receive the treatment they need.
“We have done so many high-risk liver transplants,” explains Dr. Hashimoto. “These high-risk transplants include combined cardiac surgery and liver transplant. For example, if a patient needs coronary artery bypass or heart valve replacement at the time of transplant, most centers won’t transplant. They deem these patients to be too high-risk.”
He continues, “These are super high-risk surgeries, but we have the best cardiac program in the world, and our transplant program works together with them to treat these high-risk patients.”
Cleveland Clinic also feels confident accepting medically high-risk patients because of its Medical Intensive Liver Unit (MILU). Christina Lindenmeyer, MD, is a founder and Co-Director of Cleveland Clinic’s MILU, which is one of the few intensive care units in the country dedicated to patients with acute and chronic liver failure. The MILU cares for patients who need ICU care prior to transplant by keeping them stable.
“Thanks to her leadership and close collaboration with Aanchal Kapoor, MD, who is Director of MILU, we have had significant growth and improvement in care for transplant candidates. The flow from patient referral and evaluation to transplant has become very smooth and efficient for critically ill patients who have a very small window to receive a lifesaving liver transplant,” says Dr. Hashimoto.
Advertisement
Another important evolution at Cleveland Clinic has been in the approach to alcohol-related liver disease, which has become the leading indication for liver transplantation. Historically, listing criteria required a minimum of six months of documented abstinence. However, many patients with severe liver disease were unable to survive long enough to meet this requirement. In response, the Cleveland Clinic Liver Transplant Program has adopted a more individualized and timely approach to listing, allowing selected patients to be considered for transplantation earlier in the course of their illness. To ensure that this expansion is implemented safely and responsibly, the program has established a robust multidisciplinary care model that provides comprehensive support both before and after transplantation. This effort is led by Jamak Modaresi Esfeh, MD, Medical Director of Liver Transplantation, Erin Dean, MD, lead transplant psychiatrist, along with a dedicated team of liver transplant social workers.
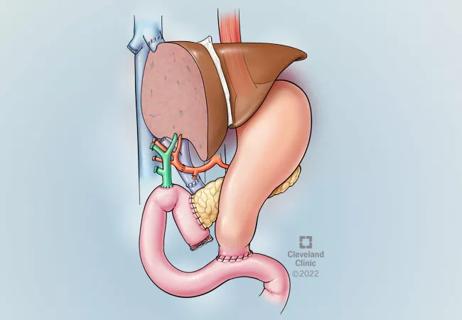
As the prevalence of metabolic dysfunction–associated liver disease continues to rise, Cleveland Clinic increasingly cares for medically complex transplant candidates with obesity, diabetes, and dyslipidemia. These patients are at higher risk for disease recurrence in the allograft, which can adversely impact long-term outcomes. To address this challenge, we have adopted a proactive, multidisciplinary strategy that includes simultaneous liver transplantation and sleeve gastrectomy in selected patients to reduce the risk of recurrence and improve postoperative metabolic health. Metabolic disease also has important implications for living donation. To expand the donor pool safely, Sobia Lique, MD, a transplant hepatologist, collaborates closely with the Cleveland Clinic Metabolic Institute to help potential living donors achieve weight loss and optimize metabolic health prior to donation.
Advertisement
Dr. Hashimoto also credits machine perfusion with helping to expand liver transplants at Cleveland Clinic.
“After the clinical trial with a home-grown perfusion pump, we started routinely using machine perfusion for donor liver preservation in 2022,” he explains. “Before 2022, we used to preserve the donor liver with cold preservation solution to minimize the metabolic activity of the liver so that the process of donor liver damage could be slowed down. Now, we can keep the liver pumped with normothermic oxygenated blood. So, you can keep the donor liver outside of the body healthy, which allows us to transplant more livers.”
There are several benefits to machine perfusion. Dr. Hashimoto suggests one of the biggest advantages is that donor liver quality can be assessed while livers are perfused on the pump.
“We check the blood perfusate and the bile to see the viability of the graft,” he says. “Prior to perfusion, many livers were discarded because they weren’t deemed viable due to “poor quality” judged by the surgeon’s experience. But with perfusion, we can now be more objective in our evaluation of organs. The use of viability assessment during machine perfusion has increased the availability of donor livers for transplantation. This innovative approach enables the transplant team to safely expand indications and reach more patients in need. Andrea Schlegel, MD, a liver transplant surgeon, leads several research initiatives focused on organ viability assessment during machine perfusion. Her work has received broad national and international recognition.
Advertisement
Rising rates of oncologic conditions that can impact liver health are also contributing to the rising recipient pool. For example, colon cancer rates have been steadily rising, and a high proportion of patients with colorectal cancer also experience liver metastasis. To improve patient care and access to transplant, Cleveland Clinic has established a multidisciplinary Liver Transplant Oncology Board led by the young leaders, Mazhar Khalil, MD, transplant surgeon, and Shilpa Junna, MD, transplant hepatologist.
“If patients have unresectable colorectal cancer with liver metastasis, the current best chemotherapy can achieve only 10% of five-year survival,” says Dr. Hashimoto. “Historically, unresectable colorectal cancer liver metastasis was an absolute contraindication for liver transplantation. However, recent studies show that liver transplantation can achieve around 60% to 70% five-year survival rate with strict patient selection.”
Cleveland Clinic has implemented a novel liver-directed treatment protocol aimed at reducing tumor burden prior to transplantation. Preliminary data suggest that this approach may decrease the risk of post-transplant tumor recurrence.
In addition to patients with unresectable colorectal cancer liver metastases, Cleveland Clinic also evaluates and treats selected patients with advanced hepatic malignancies, including unresectable hilar cholangiocarcinoma, intrahepatic cholangiocarcinoma, neuroendocrine tumor liver metastases, and hepatocellular carcinoma. The program takes a highly multidisciplinary approach, working in close collaboration with medical oncology, radiation oncology, interventional radiology, and diagnostic radiology to optimize care for these high-risk patients. With a transplant recipient pool that is expected to continue to rise, Dr. Hashimoto stresses that the roles of machine perfusion and living donor liver transplantation will become increasingly essential.
There are several goals that the Liver Transplant Program is focused on achieving in the next three years. The group hopes to expand its annual transplant number to 300 or more by 2027. They believe that with its continued and steady increase in referrals, this is a goal that is within reach.
To improve patient care quality, Cleveland Clinic Liver Transplant Program focuses on three important metrics, including pretransplant waitlist mortality rate, waiting time, and posttransplant survival. “For us, achieving low waitlist mortality and good survival after transplant is challenging because we’re taking on some of the highest-risk cases. Many other medical centers would not be willing to treat the patients that we treat. In fact, many patients who come to Cleveland Clinic have already been declined by other centers. But I believe this is our mission, and there are ways to improve our patient care.”
“One of the aspects I’m most proud of with our Liver Transplant Program is our culture,” says Dr. Hashimoto. “We have a collaborative culture — we help each other and search for and implement innovations that can improve care for our patients. I’ve been a caregiver here for over 20 years, and when I reflect on what things were like when I started to where things are today, we’ve come a long way. As always, there is still more work to be done, but I’m excited about the future of liver transplantation and transplantation at our center.”
Advertisement

Enhanced visualization and dexterity enable safer, more precise procedures and lead to better patient outcomes

Minimally invasive approach, peri- and postoperative protocols reduce risk and recovery time for these rare, magnanimous two-time donors

Patient receives liver transplant and a new lease on life

New research shows dramatic reduction in waitlist times with new technology

Cleveland Clinic study shows positive outcomes for donors and recipients

Program's approach maximizes donor safety without compromising recipients' outcomes

Program expands as data continues to show improved outcomes
Atypical cells discovered after primary sclerosing cholangitis diagnosis