Locations:

Even young patients with high activity demands can benefit
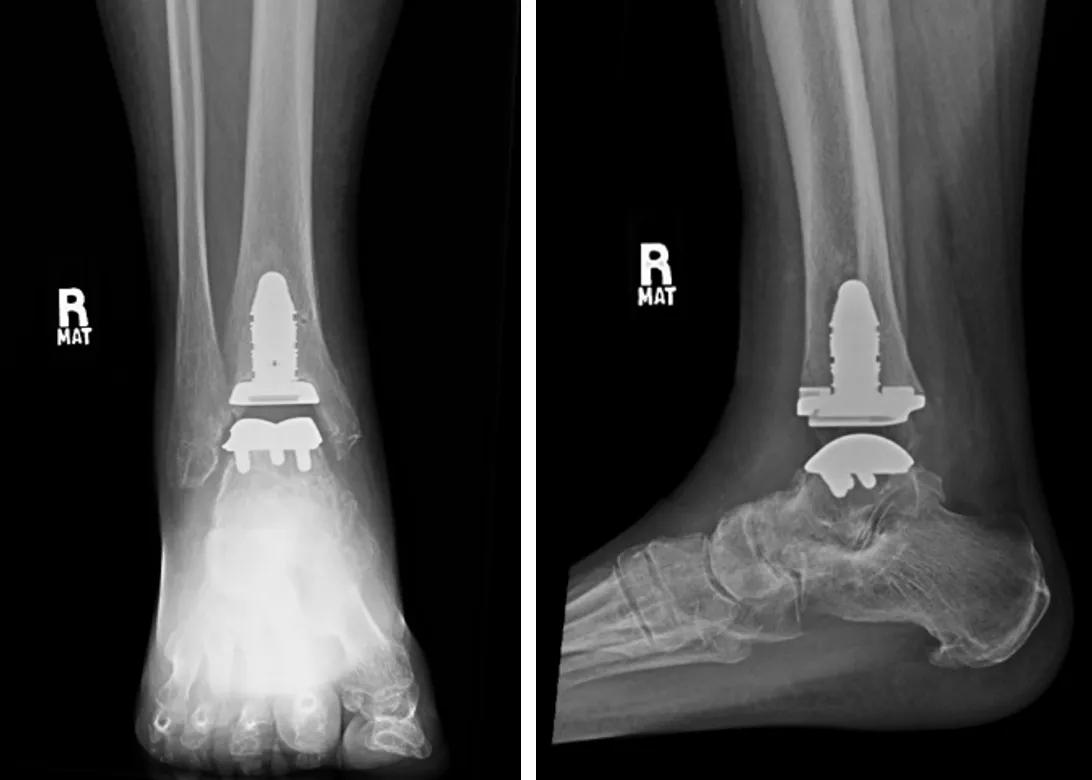
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ddda5fc4-2054-46a9-99f0-8792e2f13f9b/total-ankle-replacement-xray1)
Total ankle replacement
Total ankle replacement (TAR) was introduced in the 1970s, but initial design flaws led to significant failures. As a result, ankle fusion continued to be the gold standard in treating ankle arthritis.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In the 1990s and early 2000s, the current generation of TAR implants was approved by the U.S. Food and Drug Administration and brought to market. These implant designs produced much better outcomes and survivorship rates, and mainstream use of TAR increased. Between 1998 and 2010, use of TAR increased sixfold while ankle fusion remained constant.
With TAR now a successful option for patients seeking to preserve motion, surgeons must be aware of both the indications and contraindications for the procedure. As with total hip and knee replacement, patients with end-stage arthritis are candidates for the surgery. Surgery is considered only after trialing nonoperative treatments, such as NSAID medications, activity modification, bracing, anti-inflammatories, injections and shoe-wear modifications.
“Although conventionally TAR was seen as ideal for older patients without ankle or foot deformity and with lower activity demands, this is no longer the case,” says Sagar Chawla, MD, a Cleveland Clinic orthopaedic surgeon specializing in foot and ankle disorders. “With the latest implants and techniques, we routinely treat younger patients with high activity demands and patients with concomitant ankle and foot deformity.”
Absolute contraindications to TAR are:
Relative contraindications are:
Advertisement
In evaluating a patient for TAR, a medical history is recorded, and a standard physical is completed, paying close attention to alignment and neurovascular exam. Weight-bearing foot and ankle films are standard to assess the alignment of the ankle joint as well as the status of the surrounding joints. Routinely, advanced imaging in the form of a CT scan is obtained to better evaluate the bony architecture.
A detailed discussion with the patient should include the risks and benefits of both TAR and ankle fusion, Dr. Chawla says.
The majority of ankle replacements are performed with an anterior ankle approach. If the patient has concomitant foot and/or ankle deformities that need to be addressed at the same time, there may be additional incisions. The surgery typically takes two to three hours and can be performed as an outpatient procedure, although many patients spend one night in the hospital.
“Patients are typically non-weight-bearing for four to six weeks after surgery,” Dr. Chawla says. “Most patients return to daily activities within three months. Athletic activities take more time. Most patients return to tennis and golf within six months, for example.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ddda5fc4-2054-46a9-99f0-8792e2f13f9b/total-ankle-replacement-xray1)
Stemmed total ankle replacement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7c92dc95-54a2-4a3f-812c-d84b309e1a81/total-ankle-replacement-xray2)
Nonstemmed total ankle replacement
Current data show that patients who undergo TAR have improved patient-reported outcomes and decreased pain after surgery and achieve a 30- to 40-degree arc of motion, on average. Similar to data on total knee replacement, patients with more severe radiographic arthritis and worse function preoperatively have greater improvement after TAR compared to patients with less severe arthritis and better baseline function.
Advertisement
When comparing TAR to ankle fusion, data are mixed. Most studies report that patients undergoing TAR have slightly better patient-reported outcomes and a better gait but a higher risk of reoperation compared to patients having ankle fusion. However, there are studies that have shown no difference between the two surgical options, Dr. Chawla notes.
“In my practice, I typically perform TAR unless there is a contraindication or the patient prefers ankle arthrodesis,” he says. “For patients with a significant deformity of the ankle or foot, I occasionally perform two-stage surgery. The first stage is deformity correction followed three to four months later by TAR.”
In conclusion, TAR is a successful option for patients with end-stage ankle arthritis. Although there are contraindications, most patients are candidates. Surgeons should discuss the risks and benefits of both TAR and ankle arthrodesis with patients who are candidates for TAR.
Advertisement
Advertisement

Arthrodesis is not the only surgical option

PTs’ roles as educators and translators make them a natural fit for informatics

Innovative procedure offers less-invasive alternative to Latarjet procedure

Even patients with reported penicillin allergies can receive it without increased complications

Study challenges assumptions about risk evaluation in total hip revision

Protein expression in synovial fluid indicates patients’ immune factors may be involved

Cleveland Clinic’s Global Peak Performance Center and PGA TOUR partnership pair advanced assessment with longitudinal follow-up to enhance clinical decision-making

Study highlights the need for objective functional measures as value-based care expands