Locations:

Consensus statement outlines the team, infrastructure and experience needed to deliver TTVI safely and effectively
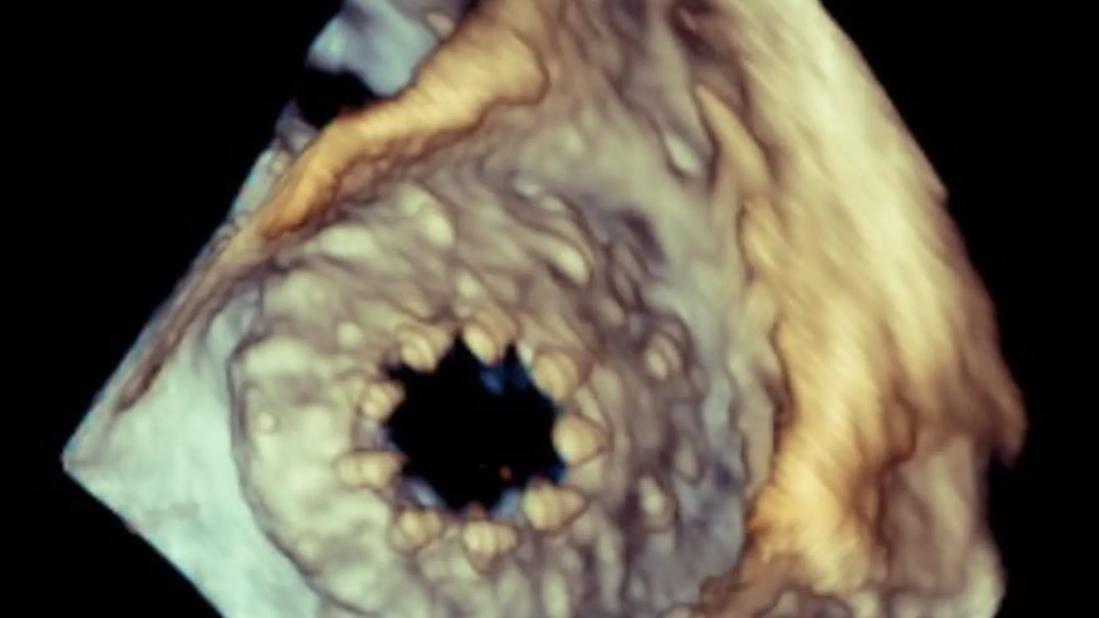
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/eb675a2f-6534-4a27-83a2-55611dea3d19/Transesophageal-echocardiogram-tricuspid-valve-replacement)
Tricuspid valve after transcatheter replacement
As transcatheter therapies for tricuspid regurgitation become more widely available, the question is no longer how these procedures can be performed but which centers and teams are best equipped to deliver them safely and effectively.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A new consensus statement published by the American College of Cardiology, American Heart Association and partnering societies addresses that question directly. The document outlines the core elements of a transcatheter tricuspid valve intervention (TTVI) program, emphasizing multidisciplinary evaluation, institutional and operator readiness, and outcomes tracking.
The EVOQUE transcatheter tricuspid valve replacement system from Edwards Lifesciences and the TriClip™ transcatheter edge-to-edge repair system from Abbott have expanded treatment options for patients with severe tricuspid regurgitation, particularly those with high surgical risk. Approved by the FDA in 2024 as breakthrough devices, these technologies quickly became accessible based on limited clinical evidence.
Soon after, U.S. regulatory processes changed, streamlining how these breakthrough devices moved from FDA approval to Centers for Medicare & Medicaid Services (CMS) coverage. As part of these changes, the FDA requires device manufacturers in the new TAP program to monitor and report patient outcomes themselves to maintain device approval. As such, the rollout of EVOQUE and TriClip devices now is driven by manufacturer-led training and site selection, not formal CMS standards for clinicians and hospitals.
“We began writing the consensus statement to help inform CMS national coverage determination on the new TTVI devices,” says coauthor Samir Kapadia, MD, Chair of Cardiovascular Medicine at Cleveland Clinic. “Before we finished, the FDA and CMS introduced a new process that no longer relies on input from a document like this. CMS now issues a proposed national coverage determination on the same day the FDA grants marketing approval. While this new process allows for rapid dissemination and greater patient access, there’s less clarity around who should be performing these procedures.”
Advertisement
He adds that in the absence of formal requirements, the writing group felt it was important to define the resources, experience and quality safeguards needed for safe TTVI adoption.
Published in the Journal of the American College of Cardiology (2026 Mar 25:S0735-1097(26)05481-1), the multisociety statement is the result of broad collaboration and rigorous review.
Below are five key takeaways for heart surgeons and cardiologists, as highlighted by Dr. Kapadia.
The statement makes clear that TTVI should not be approached as a stand-alone procedure performed by an individual operator. Patients with severe tricuspid regurgitation often present with complex anatomy, advanced right-sided chamber remodeling, pulmonary hypertension, renal or hepatic dysfunction, cardiac implantable devices or lead-management issues.
Accordingly, the statement recommends evaluation by a multidisciplinary team with expertise in cardiology, cardiac imaging, interventional cardiology, cardiac surgery and electrophysiology.
Additional specialists should be involved as needed, including heart failure specialists, anesthesiologists, and hepatology or nephrology specialists.
The team’s role includes patient assessment, optimization before intervention, procedural planning, intraprocedural imaging guidance, management of rhythm-device issues and long-term follow-up.
“Multimodality imaging is central to TTVI because procedural success depends on accurate characterization of tricuspid regurgitation mechanism and severity, annular dimensions, leaflet anatomy, right ventricular function, venous anatomy and device-lead interactions,” says Cleveland Clinic cardiovascular imaging specialist Rhonda Miyasaka, MD. “Additionally, an interventional echocardiographer is essential for providing guidance as a device is being implanted.”
Advertisement
A TTVI program requires more than device access. It requires an established structural heart platform, surgical backup, advanced imaging capability and electrophysiology support. Although CMS has not established formal thresholds for TTVI, the consensus statement argues that institutional experience remains an important marker of readiness.
“When TAVR [transcatheter aortic valve replacement] was first approved, there were specific CMS criteria defining which hospitals and operators could perform it,” Dr. Kapadia says. “For tricuspid valve devices, the approach is very different and there are no CMS criteria. The volume thresholds we propose aren’t based on tricuspid-specific data, but rather on experience with mitral therapies and our understanding of the learning curve.”
The statement recommends that centers establishing a TTVI program have:
“These criteria are intended less as rigid requirements than as markers of whether a center has the program maturity to launch a TTVI service responsibly,” Dr. Kapadia says.
Advertisement
Adds Cleveland Clinic cardiothoracic surgeon Tarek Malas, MD: “Patients with tricuspid valve disease are often very complex, requiring multidisciplinary involvement and top-end imaging. Our structural program has led the way in this very dynamic and evolving field. Our function relies on expertise from surgeons, cardiologists and imaging specialists and the essential infrastructure to make a tricuspid structural program a success.”
The statement recommends that catheter operators and interventional echocardiographers:
“Given the steep imaging and technical learning curve in tricuspid intervention, prior experience in structural heart disease, particularly leaflet-based repair and complex transseptal or transfemoral procedures, is likely to be more relevant than device-specific training alone,” Dr. Kapadia says.
Ongoing evaluation and real-world data collection will be necessary to support safety monitoring and ensure the long-term effectiveness of transcatheter tricuspid therapies. The consensus statement introduces a new TTVI module in the Society of Thoracic Surgeons and American College of Cardiology’s TVT Registry. Through this module, TTVI programs should submit case data, particularly procedural safety and device performance, long-term clinical outcomes, and patient-reported outcomes.
Advertisement
Maintaining quality requires sustained case volume and continued availability of the multidisciplinary team. Therefore, the statement proposes these maintenance benchmarks for centers already performing TTVI:
The authors are clear that these recommendations set a foundation for TTVI, but aren’t the final word. As evidence evolves, longer-term outcomes are reported and more devices enter the field, these recommendations will need to be updated, says Dr. Kapadia. In the meantime, the statement offers a guide to safe adoption of TTVI during a time of rapid growth.
“Institutional readiness matters,” adds Amar Krishnaswamy, MD, Section Head of Interventional Cardiology at Cleveland Clinic. “It is not just about having a device and a cath lab. It is about having the full structural, surgical, imaging, electrophysiology and recovery infrastructure needed to manage complex patients and complications. Success depends less on a single operator and more on a mature, multidisciplinary system of care.”
Advertisement

Study supports addressing mitral regurgitation before mild tricuspid regurgitation progresses

TRISCEND II trial reports 1-year results

Limited data and experience will translate to a cautious rollout
Cleveland Clinic study argues against waiting for symptoms to develop
TEER is found to be a safe and good option for severe TR in select patients
Understanding VC anatomy is critical for transcatheter tricuspid valve interventions

Join us in New York Dec. 4-5 for evidence-based instruction with real-world examples

Why Cleveland Clinic is launching its cardioimmunology center