Locations:

Cleveland Clinic experience points to a symptoms- and complications-based approach
For patients with an aberrant right subclavian artery (ARSA), decisions on whether to intervene are best individualized based on the presence or absence of symptoms and complications. So concludes a review of Cleveland Clinic’s recent experience with ARSA, which notes that asymptomatic patients whose ARSA is nonaneurysmal may not need intervention and can be safely monitored with serial imaging. The study was published in the Journal of Vascular Surgery (2022;75:1343-1348).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“A key challenge of ARSA management has been the absence of standardization in how to measure ectatic or aneurysmal disease presentations and in the indications for intervening in patients without symptoms,” says Cleveland Clinic vascular surgeon Francis Caputo, MD. “In view of the paucity of studies on ARSA treatment, a team from our Department of Vascular Surgery set out to review our experience in treating patients with this entity and the indications for surgical repair.”
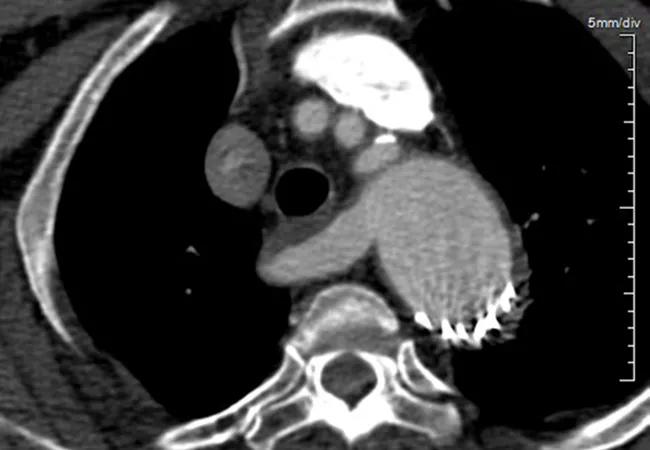
ARSA (depicted in the image above) is a surprisingly common anomaly of the aortic arch, reported in approximately 1% of the general population. It occurs as a result of abnormal entanglement of the aortic anatomy that causes the right subclavian artery to arise from the descending thoracic aorta just distal to the left subclavian artery. Variations in precisely where the aberrant artery ends up passing can result in a variety of clinical presentations.
Literature to date suggests that ARSA displays a slight female preponderance and is asymptomatic in most patients. Symptoms most frequently appear around age 50, with the most common being dysphagia, dyspnea and chest pain.
When ARSA’s origin is ectatic or aneurysmal, it is known as a Kommerell diverticulum. Literature reports indicate that 20% to 43% of ARSA cases involve Kommerell diverticulum, the Cleveland Clinic study authors note.
The researchers reviewed the records of all Cleveland Clinic patients with an ARSA diagnosis over a recent 11-year period (2009-2019). Patients’ CT scans were retrospectively analyzed, with aortic and ARSA diameters measured at 10 distinct segments. Demographic data and information on comorbidities and operative interventions were compiled.
Advertisement
Of the 32 ARSA patients identified, two had insufficient imaging studies, leaving 30 patients for inclusion in the analysis. This group was 57% female and had a mean age of 54.5 years.
Two-thirds of the cohort (20/30) had undergone surgical repair at presentation, with the remaining 10 patients initially managed with observation. Of these 10 patients, four later required intervention, which resulted in a total of 24 operative interventions across the cohort. Thirteen (54%) of these procedures were hybrid interventions that involved right carotid/subclavian bypass or transposition and thoracic endovascular aortic repair. The average follow-up of patients who were observed was 4.1 ± 3.5 years.
Key findings of the analysis include the following:
Advertisement
Dr. Caputo notes that a majority of patients who were managed with observation did not develop symptoms or require intervention throughout four-year follow-up period. “This suggests that patients with an aberrant subclavian right artery with normal contours and no evidence of ectasia or aneurysmal degeneration may not need intervention in the absence of symptoms,” he observes, “although annual serial imaging surveillance is certainly indicated.” He adds that prospective data are needed to establish this more definitively, however.
The finding that aortic and ARSA cross-sectional diameters did not differ between the intervention and observation groups supports an approach to intervention based primarily on symptoms or aorta-related complications, the study authors contend. Additionally, they note that measuring the ARSA diameter 1 cm distal to the ostium of the vessel could be a helpful guide in monitoring vessel diameter changes.
“But more research is needed before we can identify size criteria for when operative repair of an asymptomatic Kommerell diverticulum is indicated,” Dr. Caputo says.
“Patients with aberrant right subclavian artery are often asymptomatic and intervention is based on growth and size,” notes Cleveland Clinic cardiothoracic surgeon Patrick Vargo, MD, who was not involved in the study. “In those patients with normal-caliber subclavian arteries and dysphagia, a comprehensive swallowing evaluation is important to identify other causes.”
Advertisement
Advertisement

How Cleveland Clinic is using and testing TMVR systems and approaches

NIH-funded comparative trial will complete enrollment soon

How Cleveland Clinic is helping shape the evolution of M-TEER for secondary and primary MR

Optimal management requires an experienced center

Safety and efficacy are comparable to open repair across 2,600+ cases at Cleveland Clinic

Why and how Cleveland Clinic achieves repair in 99% of patients

Multimodal evaluations reveal more anatomic details to inform treatment

Insights on ex vivo lung perfusion, dual-organ transplant, cardiac comorbidities and more