Locations:

Most are slow-growing and can safely be monitored every three years
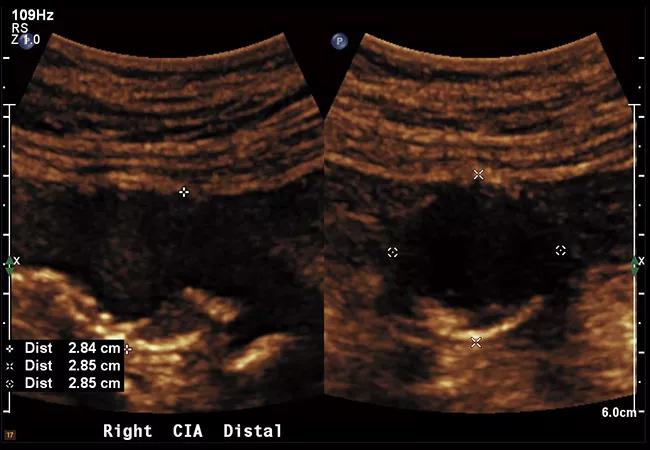
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/70c81b0f-357d-4c60-9c87-746b2a0122d1/22-HVI-2730358-CQD-650x450-1_jpg)
22-HVI-2730358 CQD 650×450
Most small abdominal aortic aneurysms (AAAs) and isolated common iliac artery aneurysms (CIAAs) can safely be monitored every three years with duplex ultrasound, with larger ones needing more frequent surveillance. So conclude clinician researchers from Cleveland Clinic in the wake of two studies they recently published on aneurysm surveillance and management — one on CIAAs in the Journal of Vascular Surgery and the other on small AAAs in the Annals of Vascular Surgery.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“The current recommendations from professional societies are based on a large amount of low-quality data and information from older databases,” says Cleveland Clinic vascular surgeon Jarrad Rowse, MD, lead author of the study on small AAAs and a co-author of the study on CIAAs. “We follow a large number of patients with these aneurysms, which gave us the opportunity to investigate this population further. These studies provide strong support for current society guidelines, with some refinements.”
Isolated CIAAs — i.e., those not associated with a concomitant AAA — are rare, constituting only about 7% of all aortoiliac aneurysms. There is currently no well-defined surveillance regimen for monitoring them and no consensus on optimal size for performing elective repair. The European Society for Vascular Surgery recommends monitoring every three years for CIAAs 2.0 to 2.9 cm in diameter, and annually for larger ones.
“Current practice recommendations are extrapolated from the more ample abdominal aortic aneurysm data,” says Sean Steenberge, MD, MSc, a surgeon in Cleveland Clinic’s Department of Vascular Surgery and first author of the study on CIAA surveillance. “We believe our study is the largest published single-center series specifically focused on isolated common iliac artery aneurysms.”
Study design. The investigators reviewed duplex ultrasound and CT imaging of 244 isolated CIAAs (≥ 2.0 cm in diameter) among 167 patients (average age, 68.1 years; 94% male and 91% white) from 2008 to 2020.
Advertisement
Findings. More than two-thirds of the aneurysms were first identified with duplex ultrasound, with the rest by CT imaging. Aneurysm surveillance was performed by a combination of CT and ultrasound imaging in 57% of cases, and by serial ultrasound alone in 43%. Average length of follow-up was 62.1 ± 40.1 months, during which 19 patients (11%) underwent operative repair, with the average aneurysm diameter at the time of repair being 3.3 ± 1.02 cm. No aneurysms were symptomatic or ruptured at time of identification or during follow-up.
Two patients who had been lost to follow-up for several years after an initially discovered isolated CIAA were later found to have had unusually rapid aneurysm growth (0.5 to > 1 cm per year) in the subsequent years.
Recommendations. To detect a rare, rapidly growing isolated CIAA, the authors recommend conducting a follow-up imaging study one year after initial isolated CIAA identification for all patients. Thereafter, they endorse the following aneurysm monitoring regimen with duplex ultrasound or CT angiography (CT angiography is recommended to confirm ultrasound results when diameter reaches 3.0 cm), based on growth rates found in the study:
Advertisement
Full aortic surveillance is recommended every five years.
“We recommend elective repair when the diameter reaches 3.5 cm,” says Dr. Steenberge. “But additional data are needed to strengthen that guidance.”
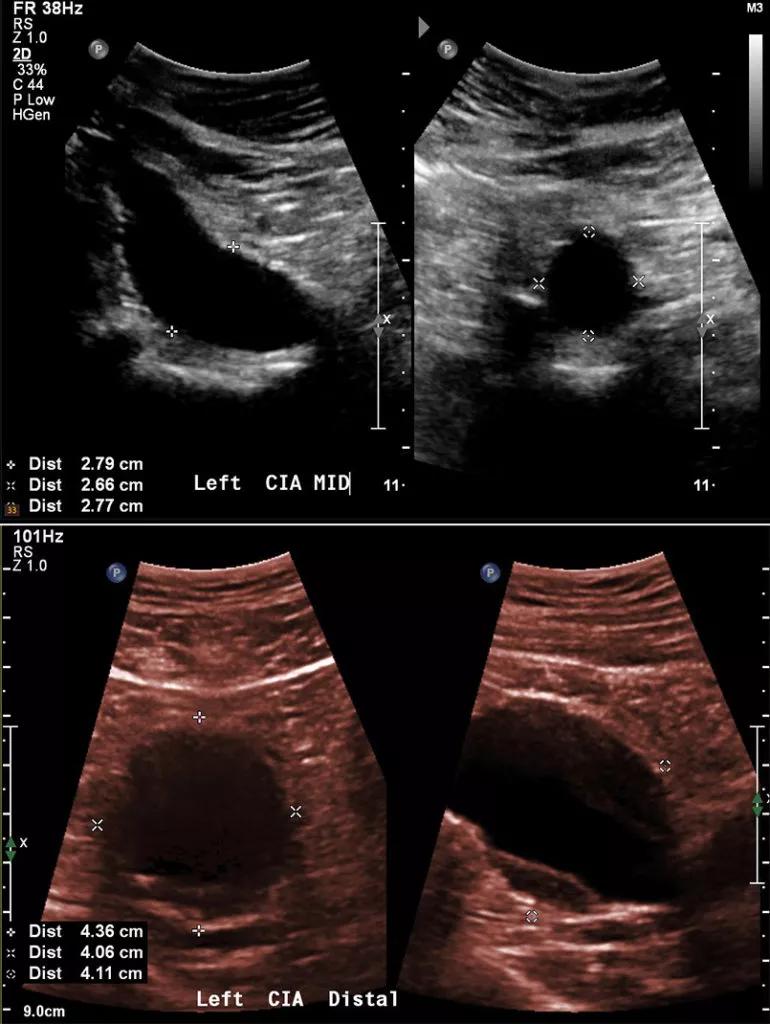
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/820da9b4-5678-492c-af10-a6fef94d06d4/22-HVI-2730358-CQD-Inset-1-770x1024_jpg)
Ultrasound images of isolated CIAAs with diameters of 2.7 cm (top panel) and 4 cm (bottom panel).
Current Society for Vascular Surgery guidelines for monitoring small AAAs — every three years for aneurysm diameters of 3.0 to 3.9 cm, and annually for diameters of 4.0 to 4.9 cm — are based on low-quality evidence and provide no patient-specific guidance.
Study design. The population of the study on surveillance of small AAAs — patients with a baseline AAA diameter of less than 5.0 cm who had at least two ultrasounds — was identified from Cleveland Clinic records from 2008 to 2018. There were 1,581 patients (mean age, 73 years; 78% male and 93% white) and nearly 6,000 ultrasounds, with a mean follow-up of 28 months.
Findings. Average annual maximum diameter growth rates were found to be 0.18 cm for AAAs with a diameter of 3.0 to 3.9 cm and 0.36 cm for those with a diameter of 4.0 to 4.9 cm (P < 0.001 for the difference).
Growth rates varied considerably, with 68.2% of patients having no growth over the observed time period, 21.6% having expected growth and 10.2% having rapid growth.
Patient-specific factors. Patients who were male and had a baseline AAA size of 4.0 to 4.9 cm were more likely to have rapid growth (P = 0.002) and to undergo eventual repair (P < 0.001). Patients taking metformin were more likely to have no aneurysm growth (P < 0.05).
Advertisement
Recommendations. The authors write that their findings support the following surveillance schedule:
“Unlike in other studies, we did not find that small aneurysms grew faster in women,” Dr. Rowse notes. “However, the cohort was too small to make definitive recommendations for women, so more study is needed to clarify their optimal surveillance strategy.”
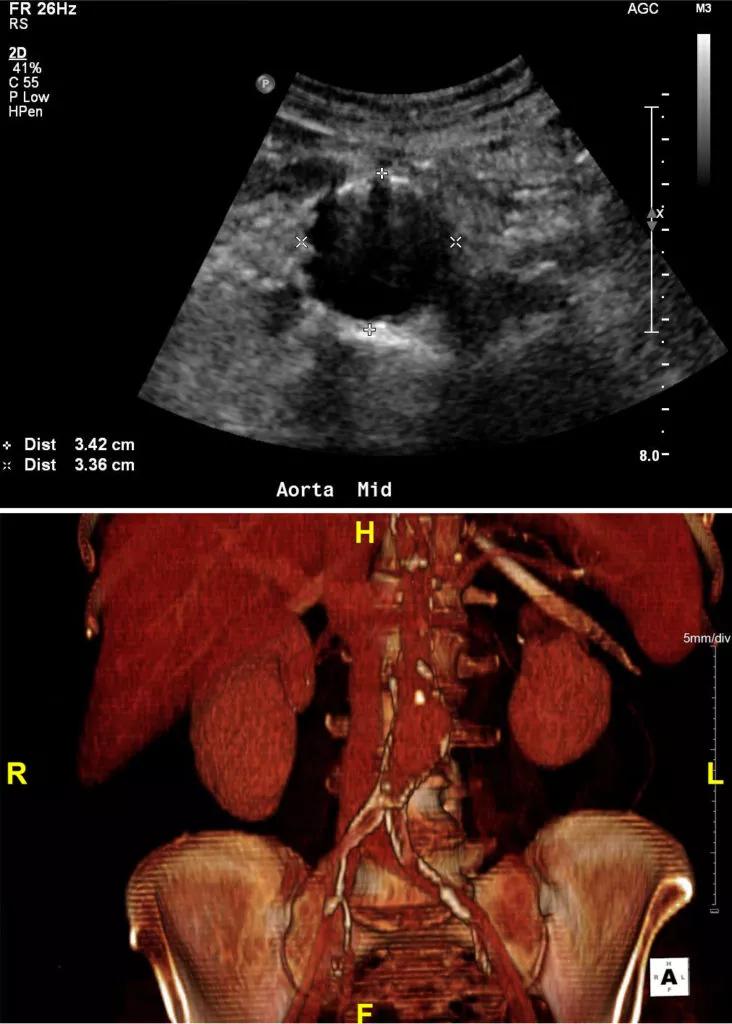
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1a8b89fb-91cd-4493-9b7e-283d9616f4b7/22-HVI-2730358-CQD-Inset-2-732x1024_jpg)
Two imaging studies of small AAAs — an ultrasound on the top and a 3D CT reconstruction on the bottom.
Advertisement
Advertisement

‘Sac flow’ is more precise and will ease unfounded patient concerns, experts argue

Join us in New York Dec. 4-5 for evidence-based instruction with real-world examples

First-ever transcarotid artery revascularization trial with no strokes or device-related deaths

Consensus statement outlines the team, infrastructure and experience needed to deliver TTVI safely and effectively

Innovative approach to living-tissue AVR achieves low reintervention rates, excellent long-term survival

Diagnosis and treatment of malnutrition and cachexia are key to improving cardiac outcomes

Symptom burden at presentation is a potent predictor of long-term survival, large analysis shows

New framework better distinguishes stable from critically ill patients