Locations:

Insights from the Cleveland Clinic experience and a multispecialty alliance

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/dfc6c4e3-1f6e-4814-b7e2-9b11006b75bd/mesh-stent-in-carotid-artery)
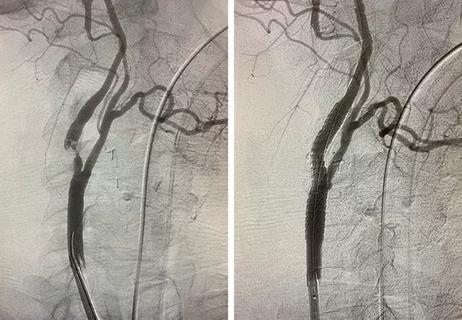
mesh stent in a carotid artery
When the Centers for Medicare & Medicaid Services (CMS) announced its national coverage determination (NCD) on carotid artery stenting last fall, it brought new options for clinicians and patients as well as new responsibilities for providers and health systems.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“The NCD basically stated that carotid artery stenting (CAS) — whether transfemoral CAS or transcarotid artery revascularization (TCAR) — would be considered equivalent to carotid endarterectomy (CEA) for reimbursement purposes for patients on Medicare,” says Sean Lyden, MD, Chair of Vascular Surgery at Cleveland Clinic. “That is liberating because now we don’t need to have awkward conversations with patients about what their insurance is before discussing treatment options. But the change also stirred up questions about how providers and hospitals should adapt to this new landscape in terms of training and accountability.”
Dr. Lyden received many such questions from colleagues around the nation, in view of his role at a leading medical center like Cleveland Clinic and as a member of the Multispecialty Carotid Alliance, a national group of interventional cardiologists, vascular medicine physicians, vascular surgeons, neurologists, neurosurgeons and interventional neurologists promoting awareness and education to reduce stroke from carotid artery disease. This article addresses many of those questions by sharing actions taken by the Multispecialty Carotid Alliance and Cleveland Clinic to improve care delivery for carotid disease in the wake of the recent NCD.
Prior to the 2023 NCD, CMS would reimburse for CAS in a Medicare beneficiary only if the patient was deemed at high surgical risk from CEA and the lesion was symptomatic (causing amaurosis fugax, transient ischemic attack or nondisabling stroke) and greater than 70% stenosed. The result is that only about 5% of patients needing intervention for carotid artery disease ended up undergoing a CAS procedure.
Advertisement
Under the new NCD, CMS will cover the two stenting procedures — transfemoral CAS and TCAR — under the same conditions that it covers CEA, namely:
The NCD further specifies that carotid ultrasonography should be the first diagnostic test to show whether a lesion is present. If revascularization is considered, CT angiography or MR angiography should be performed to confirm the location and extent of stenosis as well as anatomical factors that may impact the best option for a patient. The treatment choice must be the result of shared decision-making with the patient that includes discussion of risks and benefits of all treatment options, including optimal medical management.
“We know that some patients are best suited to one of the three options — CEA, TCAR or transfemoral CAS — and that others would do fine with any of the options,” Dr. Lyden says. “You just need to discuss the pros and cons of each with the patient and then together decide which is best for their individual situation.”
“From the neurological and neurosurgical perspectives, this is an important advancement,” adds Mark Bain, MD, a vascular neurosurgeon in the Cerebrovascular Center in Cleveland Clinic’s Neurological Institute. “In our Cerebrovascular Center, we value the ability to have the best expertise in all techniques available and to make the decision about which procedure is best for a particular patient without being restricted by insurance eligibility.”
Advertisement
“The innovation and entrepreneurial spirit of a Cleveland Clinic physician, in collaboration with many cross-specialty colleagues, pioneered the paradigm of carotid stenting years ago,” notes Cleveland Clinic interventional cardiologist Christopher Bajzer, MD. “The same collaboration and collegiality helped give birth to the specialty of interventional neurology. It is very satisfying to see years later that this treatment strategy is recognized by CMS as a valued option for a wider segment of patients with carotid disease. Having this as a treatment option can make all the difference to an individual patient and their family.”
The NCD’s expansion of the covered patient population means that more carotid stenting procedures will be performed in the months and years ahead than ever before.
“Many physicians stopped doing carotid stenting or never got trained in it because there weren’t enough cases to be done in the absence of CMS coverage,” Dr. Lyden says. “A lot of people need to figure out how to get trained again, and some authoritative group has to come forward with guidance on what adequate training involves and how to ensure good outcomes over time.”
The various specialties involved — vascular surgery, interventional cardiology, neurosurgery, interventional neurology — have differing guidance documents on these issues, and there is no unified statement from societies in these specialties that hospital medical executive committees can use to guide policy adoption in the wake of the NCD.
Advertisement
That’s where the Multispecialty Carotid Alliance comes in. Prior to the NCD, this group of physicians developed a white paper detailing data relevant to the status of carotid stenting in the U.S. for consideration by CMS during the NCD process. Now the alliance, which can act more nimbly than most medical or surgical societies, is working with such societies, along with industry, to explore whether consensus guidance can be developed on appropriate requirements for training and outcomes accountability related to carotid stenting.
In the near term, the alliance also is working to create educational pathways to facilitate training in carotid stenting among interested physicians and trainees in the relevant specialties. This includes collaboration with specialty societies such as the Society for Cardiovascular Angiography & Interventions (SCAI), which is offering a course on carotid stenting at its annual scientific sessions in early May. The alliance is advising SCAI on what’s essential to include in the course for current training on these procedures.
Dr. Lyden says that while the Multispecialty Carotid Alliance may eventually issue guidance on optimal policy for training and outcomes accountability around carotid stenting, probably as another white paper, for now they are focused on ensuring high-quality training for interested clinicians. “That’s where the demand and need are,” he says. “Plus, we’re likely to learn things from the initial rollout of training that can ultimately inform a document like that in a constructive way.”
Advertisement
As alliance members meet with various societies and industry players, they aim to keep the focus on the big picture. “Everyone is wondering how the NCD is going to change the landscape of how patients with carotid disease are treated,” Dr. Lyden says. “We’re trying to remind people that it’s not about how the relative numbers for each therapy change. It’s about whether shared decision-making is happening and whether operators are meeting and maintaining their outcomes. The end goal is the outcomes. It’s not about one therapy or the other. All three — CEA, transfemoral CAS and TCAR — will have a role.”
At Cleveland Clinic, soon after the NCD was issued, Dr. Lyden met with his counterparts in the relevant specialties beyond his vascular surgery team — i.e., interventional cardiology, neurosurgery and interventional neuroradiology.
These four service lines that perform carotid procedures had already been meeting monthly for years at Cleveland Clinic to discuss interesting cases and share best practices. They also met quarterly to review outcomes to ensure compliance with outcome targets. “We were already holding all four service lines accountable to the same outcome goals,” Dr. Lyden says, “so there was a single quality bar for everyone.”
The service line leaders used their post-NCD meeting to promote ongoing consensus and internal collaboration on carotid disease care, and to ensure standardization of care practices in alignment with societal guidelines across Cleveland Clinic. Most notably, they standardized their training requirements for any provider who wished to offer transfemoral CAS, in anticipation of the increased demand for this stenting procedure. “Previously, we had different requirements for how many carotid stenting cases a physician needed to perform before obtaining privileges to offer transfemoral CAS,” Dr. Lyden explains. “After discussion and consulting our individual guidance documents, we agreed to 25 cases as the threshold for privileging across the board.”
“From the quality perspective, our Comprehensive Stroke Center designation requires that we uphold the highest standards of care, quality and outcomes, regardless of which specialty is performing the procedure,” notes interventional neurologist M. Shazam Hussain, MD, Director of Cleveland Clinic’s Cerebrovascular Center. “It’s been an excellent collaboration among all of us, coming together to standardize practice and monitor safety, quality and outcomes to ensure we provide the best care to our patients.”
Dr. Lyden believes this type of consensus and collaboration among all relevant service lines is key to offering optimal carotid revascularization services for all hospitals and health systems in the wake of the recent NCD.
“You need to get all the players together to agree on credentialing requirements for doing these procedures and how to hold physicians accountable for outcomes,” he says. “And best practice is for these players to continue to meet to review outcomes by individual and by specialty to make sure outcomes are in line with goals. This can be done in keeping with a hospital’s existing medical executive committee and peer-review processes. If these things are done and patients are experiencing good outcomes and not having strokes, the type of procedure they’re getting becomes irrelevant.”
Nevertheless, he recognizes that competition among specialties exists everywhere, although he notes that this is an opportunity to use it constructively. “My field of vascular surgery has traditionally felt that carotids were our thing,” he says, “so some resistance is natural. But we’ve seen minimally invasive procedures find a place in other areas of our practice — such as thoracic aortic conditions and lower extremity conditions — and we’ve adopted those procedures as important therapy options we can offer along with open procedures.” He says that, in the same way, if vascular surgeons adopt TCAR and transfemoral CAS into their practice, they have no reason to fear losing their place in the management of carotid disease.
“There’s no physician I know who doesn’t care about quality,” Dr. Lyden concludes. “If organizations make quality and outcomes in carotid care their North Star, the rest will take care of itself.”
Advertisement

First-ever transcarotid artery revascularization trial with no strokes or device-related deaths
A look at where TCAR and transfemoral carotid stenting are likely headed
Retrospective findings from an executive health program spur interest in broader studies

JACC review calls for CMS to update coverage decision

Findings promise to shape future antiplatelet drug development and treatment strategies

How and why we're offering robot-assisted options for a full array of cardiac operations

Insights on common questions from referring providers

A snapshot of key stats from one of the world's busiest centers