Locations:

JAMA study adds new data to decades-long guidance

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/68cb67cb-bf1b-437e-a067-e32cf123418b/LQTS-sports-participation)
Boys on sports team
Patients with hypertrophic cardiomyopathy (HCM) historically have been advised against vigorous physical activity out of concern for ventricular arrhythmia that could lead to sudden cardiac arrest. A multicenter study published in JAMA Cardiology upends that conventional thinking and may provide a path toward updated clinical guidance.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The findings from a prospective cohort of 1,660 patients across 42 high-volume centers show that patients with HCM (or those with a positive genotype) who engage in vigorous exercise were no more likely to experience a life-threatening arrhythmia than those reporting moderate or sedentary activity.
Bradley Marino, MD, MBA, a study co-author and the Chief of Cardiology and Cardiovascular Medicine at Cleveland Clinic Children’s, says this landmark study could mark a shift in less conservative management of patients with HCM. It also changes the conversation between patients with HCM and their physicians when it comes to informed shared decision-making about their lifestyle and activity choices.
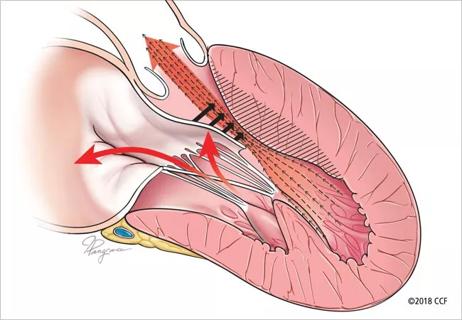
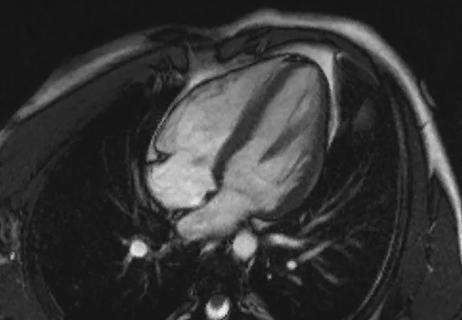
HCM, which affects about 1 in 500 individuals worldwide, is characterized by left ventricular hypertrophy. Conventional knowledge of the disease has been that rigorous activity could activate a sympathetic outflow, stimulate a ventricular arrhythmia and result in sudden cardiac death.
Over the past four decades, undiagnosed HCM has been linked to sudden cardiac death in younger individuals, particularly in those who participate in competitive sports or rigorous activity. This has led to stricter guidance, including U.S. and European consensus guidelines that have long recommended avoidance of vigorous recreational physical activity and exclusion from competitive sports for those with known disease — despite limited evidence to support this guidance.
More recently, guidelines have loosened for mild- to moderate-intensity exercise in this patient population, indicating a shift in how patients and cardiologists are approaching the conversation. Studies have underscored the benefit of physical activity in patients with HCM, who may be more likely than the general population to have obesity as well as heightened anxiety and emotional instability.
Advertisement
“So many clinicians have been challenged by their patients who wish to participate in recreational activity and competitive sports,” says Dr. Marino. “Would vigorous exercise be more likely to result in sudden cardiac death or ventricular arrhythmia? Our study assessed that particularly important question.”
The investigators examined 1,660 study participants, ages 8 to 60. Of these, 252 (15%) reported being sedentary, 709 (43%) exercised moderately and 699 (42%) engaged in vigorous exercise. Of the vigorous exercisers, 259 (37%) participated competitively.
Less than 5% of all participants (77) reached the study end point (death, resuscitated sudden cardiac arrest, arrhythmic syncope or appropriate shock from an implantable cardioverter defibrillator), resulting in two cohorts: 44 (4.6%) who did not exercise vigorously and 33 (4.7%) who did, at rates of 15.3 and 15.9 per 1,000 person-years, respectively.
“From a quality-of-life standpoint, there are now more opportunities for patients with cardiomyopathy that previously, in attempt to safeguard the patient, may not have been advisable,” Dr. Marino says.
However, he acknowledges that the risk profile of each patient with HCM is different and the degree of risk incurred varies among patient-provider dyads. This study adds new evidence to an ongoing conversation within the cardiology community that supports more informed decision-making.
Advertisement
Advertisement

End-of-treatment VALOR-HCM analyses reassure on use in women, suggest disease-modifying potential

Cardiac imaging substudy is the latest paper originating from the VANISH trial

Vigilance for symptom emergence matters, a large 20-year analysis reveals

Phase 3 ODYSSEY-HCM trial of mavacamten leaves lingering questions about potential broader use

5% of flagged ECGs in real-world study were from patients with previously undiagnosed HCM

High composite score in myectomy specimens signals worse prognosis
Few patients report left ventricular dysfunction or heart failure after one year
Avoidance of septal reduction therapy continues while LVEF dysfunction remains infrequent