Locations:

Companion study shows apparent benefit from surgery in both primary and secondary TR
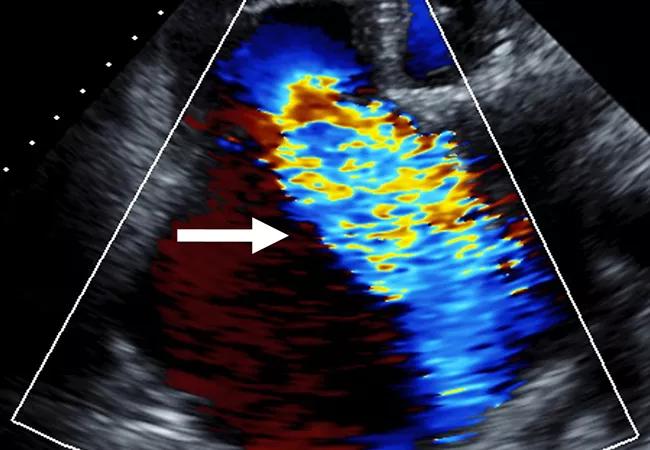
While understanding of aortic and mitral valve pathologies has progressed rapidly, the management of patients with isolated tricuspid regurgitation (TR) remains challenging. Although the condition is increasingly common, indications for intervention have not been well established, and operative mortality can be high.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Now a new Cleveland Clinic study published online in JACC Cardiovascular Imaging is helping to close the knowledge gap by shedding light on the etiologies and natural history of isolated TR in a large cohort. The researchers have also used the new information to create a risk model for predicting mortality outcomes in these patients.
“We hope this study and risk model will help guide cardiologists and cardiac surgeons on how to most effectively manage such patients,” says corresponding author Milind Desai, MD, MBA, Director of Clinical Operations in Cleveland Clinic’s Heart, Vascular & Thoracic Institute.
The observational study — the largest of its kind yet published — included consecutive patients with isolated TR entered in Cleveland Clinic’s adult echocardiography database between January 2004 and December 2018. All had isolated TR graded severe or moderate to severe by transthoracic echocardiography.
Of the 9,045 isolated TR cases identified, 94.8% were found to be secondary (pathology distorting the ventricular and/or atrial anatomy so as to impair valvular coaptation) and 5.2% were primary (pathology affecting the structural integrity of the valve). Both forms conferred adverse prognosis compared with the age- and sex-matched general U.S. population; secondary TR was associated with worse survival than primary TR in unadjusted but not adjusted multivariable analysis.
The most common etiologies of secondary TR were left heart disease (54.4%), atrial functional disease (24.3%) and pulmonary disease (17.0%). Among cases of secondary TR, those associated with pulmonary disease had the worst survival, and those related to left heart disease had significantly worse survival than those related to atrial functional disease.
Advertisement
The most common cause of primary TR was infective endocarditis (47.2%), followed by degenerative disease/prolapse (18.3%) and prosthetic valve failure (16.8%).
With the information on underlying etiology and mortality risk in hand, the authors devised a risk model to predict one-year all-cause mortality for patients with isolated secondary TR (Figure). The clinical, laboratory and imaging parameters included in the model combine for a score from 0 to 16, with increasing risk of mortality associated with rising score.
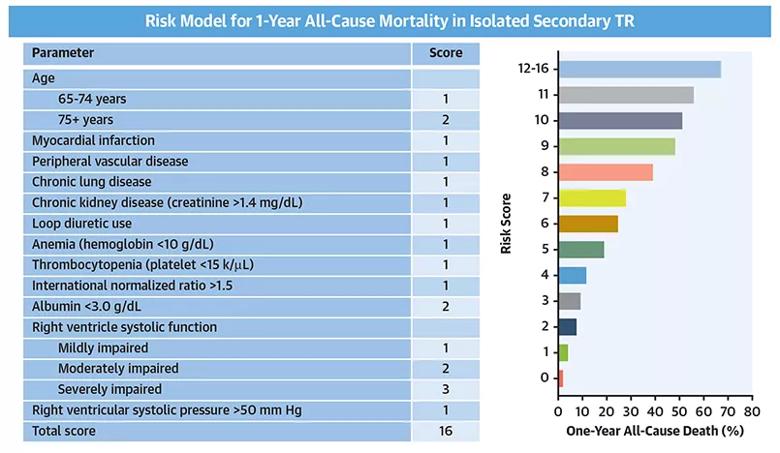
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8f50b6a2-ca37-4210-971b-5ad764453c9a/22-HVI-2623151-CQD-Inset_jpg)
Figure. Parameters used in the risk score model (left) and estimated one-year mortality rate by risk score plot (right). Reprinted from Wang et al., JACC: Cardiovascular Imaging, copyright 2021, with permission from the American College of Cardiology Foundation.
“The score stratifies mortality risk to potentially guide the management strategy for these patients,” says the study’s first author, Tom Kai Ming Wang, MBChB, MD, a cardiologist in Cleveland Clinic’s Section of Cardiovascular Imaging. “The higher the score, the worse the prognosis and therefore the greater the need to consider a surgical or transcatheter tricuspid procedure, which remain underutilized. Furthermore, optimal medical treatments tailored to underlying etiologies are important, and these etiologies include heart failure, coronary artery disease, atrial fibrillation, chronic lung disease and endocarditis.”
The novel scoring system was internally validated and is now being disseminated throughout Cleveland Clinic for use in the management of patients with isolated TR. “It’s too soon to tell whether it has affected clinical practice, but we sure hope it has,” says Dr. Desai. “We plan to share it on our website so anyone who manages valve disease can use it.”
Advertisement
Although the novel scoring system is expected to be a significant asset in the management of patients with isolated TR, it continues to undergo refinement.
“Further research is required to determine the exact threshold of risk score associated with significant risk that would benefit from intervention,” says study co-author Brian Griffin, MD, Section Head of Cardiovascular Imaging. “More research may also reveal whether there are other covariates, such as frailty or quantitative TR parameters, that can be added to further improve the model’s accuracy and be considered when managing individuals with TR.”
Even after a patient’s risk has been quantified, the optimal treatment strategy or combination of treatments remains unclear. “Randomized trials are urgently needed to compare the outcomes of surgical, transcatheter and medical therapies in patients with isolated TR,” says Dr. Desai.
Those randomized investigations may be shaped by the findings of an observational study published by the same group of Cleveland Clinic researchers in the American Journal of Cardiology (2022;162:163-169). Using the same large cohort of Cleveland Clinic patients with isolated TR from 2004 through 2018, this study analyzed outcomes according to management strategy.
Results showed that surgery was traditionally underutilized — performed in only 7% of patients overall — but steadily increased over the study period. Surgery was associated with improved survival compared with medical management alone, including after multivariable adjustment.
Advertisement
“Surgery showed a survival benefit in both primary and secondary TR,” Dr. Wang observes. “That is notable because the benefit of surgery in TR, especially secondary TR, has been considered controversial.”
Until more information is gathered, the authors conclude, patients with TR are best managed in expert valve centers to achieve the best possible outcome in view of their high risk.
“It is important to identify patients early in their disease course, particularly before they develop heart failure, to enable referral to experienced heart teams for management,” Dr. Wang notes. “As we demonstrated in another recent study (recapped in this Consult QD post), quantifying TR and right heart size and function through multimodality imaging evaluation with echocardiography and MRI parameters can be key to guiding decision-making for tricuspid procedures.”
“This new study provides an important warning that the prognosis of patients with severe TR is abysmal and TR should not be ignored,” says Amar Krishnaswamy, MD, Section Head of Invasive and Interventional Cardiology, who was not involved in the study.
“European trials and registries have demonstrated that percutaneous TR therapies are safe and effective in improving quality of life and survival,” Dr. Krishnaswamy adds. “We are fortunate that there are currently a number of minimally invasive, catheter-based options to repair or replace the tricuspid valve available at Cleveland Clinic. Unfortunately, patients with isolated TR require treatment as part of a randomized clinical trial since the FDA has yet to approve any percutaneous TR therapies. We hope that increasing data from analyses such as this one will help persuade the FDA to approve these treatments sooner rather than later.”
Advertisement
Advertisement

Scenarios where experience-based management nuance can matter most

Introducing Krishna Aragam, MD, head of new integrated clinical and research programs in cardiovascular genomics

How Cleveland Clinic is using and testing TMVR systems and approaches

NIH-funded comparative trial will complete enrollment soon

How Cleveland Clinic is helping shape the evolution of M-TEER for secondary and primary MR

Optimal management requires an experienced center

Safety and efficacy are comparable to open repair across 2,600+ cases at Cleveland Clinic

Why and how Cleveland Clinic achieves repair in 99% of patients