Locations:

Analysis of STS/ACC TVT Registry finds greatest benefit in patients with prior stroke

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a2b9714f-6407-4235-8da4-a06c54fe3f5e/22-HVI-3221311-CQD-650x450-1_jpg)
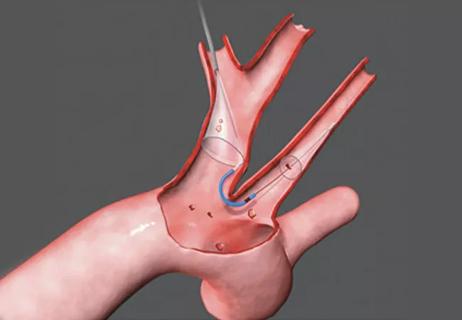
sentinel cerebral protection device capturing embolic debris
Cerebral embolic protection devices (EPDs) were developed to mitigate the risk of stroke during transcatheter aortic valve replacement (TAVR), but their benefit has not been definitively determined. Now, the largest study to date has found EPD use in TAVR to be associated with a small but significant reduction in disabling stroke but not nondisabling stroke.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The study, which used data from the Society of Thoracic Surgeons (STS)/American College of Cardiology (ACC) TVT Registry, was published in Circulation: Cardiovascular Interventions.
“These registry data are consistent with existing evidence from smaller trials and other registry data from the U.S. and other countries that generally demonstrate a reduction in clinical stroke, with the reduction in disabling stroke being the most significant,” says study co-author Samir Kapadia, MD, Chair of Cardiovascular Medicine at Cleveland Clinic.
In the PROTECTED TAVR study (N Engl J Med. 2022;387:1253-1263), a multicenter randomized trial for which Dr. Kapadia served as principal investigator, EPD use did not significantly reduce the primary outcome of periprocedural stroke, but it did lead to a statistically significant 62% relative reduction in the secondary endpoint of disabling stroke. The authors of the current analysis believed it was important to understand whether these findings could be replicated in other high-quality datasets.
They accessed STS/ACC TVT Registry data to examine the association between EPD use and disabling stroke in patients who underwent transfemoral TAVR. Disabling stroke was defined as stroke associated with either in-hospital death or discharge to a location other than the patient’s home — a definition validated by Butala et al. in a paper simultaneously published in Circulation: Cardiovascular Interventions.
Of 414,649 patients in the registry cohort, 12.9% received an EPD. The unadjusted rate of in-hospital disabling stroke was 0.7% in the EPD group and 0.9% in the no-EPD group. When instrumental variable analysis and propensity-weighted analysis were applied, EPD use was associated with a reduction in disabling stroke but not non-disabling stroke. The adjusted relative risk for disabling stroke was 0.87 (95% CI, 0.73-1.00) in the instrumental variable analysis and 0.79 (95% CI, 0.70-0.90) in the propensity-weighted analysis.
Advertisement
“The fact that the reduction in disabling stroke with EPD was smaller than reported in randomized trials may be due to this study’s retrospective nature and lack of prospective randomization,” Dr. Kapadia notes.
He adds that stroke rates in the TVT Registry are based on site reporting and that some strokes, especially more subtle ones, may be missed on routine exams. “It is clear that TAVR studies that involve the use of neurology professionals in post-procedure stroke assessment note three times more strokes than site-reported registries like TVT,” Dr. Kapadia observes. “This may also result in an underestimation of benefit from EPD use.”
Importantly, patients with prior stroke were found to derive preferential benefit from embolic protection. “In this subgroup, which makes up about 10% of all patients undergoing TAVR, embolic protection conferred a reduction in disabling stroke that was three to five times greater than for the overall study population, depending on the specific analysis conducted,” notes Dr. Kapadia.
Specifically, use of an EPD was associated with a 40% lower risk of disabling stroke among patients with prior stroke in both instrumental variable and propensity-weighted analyses. “In this subpopulation with prior stroke, the number needed to treat to prevent one disabling stroke was 155,” Dr. Kapadia observes.
Cleveland Clinic interventional cardiologists are committed to using EPDs in 100% of TAVR patients and have achieved 97% success in EPD placement, with only 3% of patients having unsuitable anatomy. The Sentinel™ Embolic Protection System, the only FDA-approved EPD to date, is used in all patients.
Advertisement
These new STS/ACC TVT Registry findings bolster the value of this practice, according to Amar Krishnaswamy, MD, Section Head of Invasive and Interventional Cardiology at Cleveland Clinic.
“It stands to reason that when 100% of patients demonstrate cerebral debris on microscopic and MRI analysis, using an EPD makes sense,” Dr. Krishnaswamy says. “Since it’s well established that the available device is safe and doesn’t increase risk in and of itself, it behooves us to use it. We have limited data on who may benefit more or less from EPD use, so it doesn’t make rational or scientific sense to be selective.”
He adds that although any stroke can be potentially devastating, the growing use of TAVR in younger patients merits special consideration for stroke protection. “The ramifications of disabling stroke are particularly high for working individuals with families,” Dr. Krishnaswamy says. “Such ramifications make it incumbent on us to make TAVR as safe as possible.”
Dr. Kapadia notes that although EPD use remains infrequent overall, high-volume centers like Cleveland Clinic tend to use EPDs because their high number of TAVR cases makes it inevitable that they see more strokes on an annual basis. “As a result, high-volume centers see the need more directly,” he says. “Also, there is often clear demand from patients. Many TAVR patients will travel to a center where EPD is routinely used because they value stroke prevention as very important.”
This observation is echoed by James Yun, MD, PhD, a cardiothoracic surgeon on Cleveland Clinic’s TAVR team. “In 2024, patients are better informed than ever before — not only about TAVR, but also the periprocedural risks,” says Dr. Yun. “In general, they are relieved to hear that our group is committed to the proactive use of EPDs, and some have sought out our center specifically because they became aware that EPDs were not used at their local hospital.”
Advertisement
The finding that patients with prior stroke benefited most from EPD use encourages research on other subpopulations, Dr. Krishnaswamy says. “There may be other groups that have higher risk and greater benefit,” he notes, “perhaps those with a bicuspid valve, those undergoing valve-in-valve TAVR or those undergoing leaflet modification.”
As for additional evidence from clinical trials, Drs. Kapadia and Krishnaswamy eagerly await the results of BHF-PROTECT-TAVI, the completed British study of patients randomized to TAVR with or without EPD. “Its data will be added to that of PROTECTED TAVR, enabling an analysis of EPD benefits in a cohort of more than 10,000 patients,” Dr. Krishnaswamy says.
Image at top shows the Sentinel™ cerebral embolic protection device. ©2022 Boston Scientific Corporation or its affiliates. All rights reserved.
Advertisement
Advertisement

Collaboration includes clinical validation of predictive modeling tool, development of second-generation tool

TVT Registry analysis could expand indication to lower surgical risk levels

Patient series and bench validation support efficacy and safety of CLEVE procedure

In the wake of NOTION-3 findings, a strong argument for physician judgment remains
Post hoc analysis of PROTECTED TAVR finds reduced stroke risk in the U.S. but not beyond

TAVR explant demands multidisciplinary expertise

How our HVTI Advisory Services team facilitated swift improvements for an allied health organization
Support for a TAVR-first approach in patients with concurrent valve and coronary disease