Locations:

Important additions to a novel surgical technique

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3e0e4cf0-03ea-4c38-af0b-a1a76be6b673/19-HRT-452-AAOCA-CQD-Hero_jpg)
19-HRT-452-AAOCA-CQD-Hero
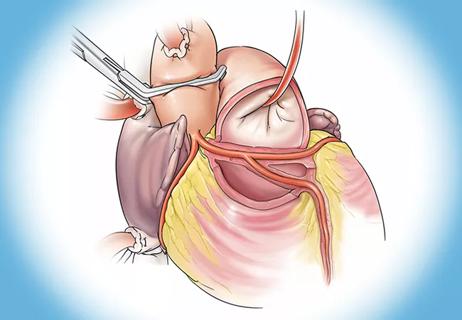
Cleveland Clinic cardiothoracic surgeon Hani K. Najm, MD, has further refined his novel surgical technique for repairing the anomalous aortic origin of the left coronary artery (AAOLCA) with transseptal course behind the right ventricular outflow tract (RVOT).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The rare AAOLCA subvariant, present in about 0.02% to 0.08% of the population, carries a high risk of sudden cardiac death. Coronary artery bypass grafting often fails, due to competitive flow. Dr. Najm’s transconal unroofing procedure, first performed in 2018 on a 40-year-old woman, offers the first opportunity for successful repair of the defect.
“Before that, there was no effective surgery for this,” Dr. Najm says.
In 2021, Dr. Najm and colleagues published positive results in seven additional patients with the “Najm procedure,” which involves transconal exposure of the left coronary artery for effective unroofing, dissection to separate the AAOLCA from the RVOT, and posterior elongation of the RVOT using an autologous pericardial patch.
Now, “as this experience has evolved, we have made important modifications in our surgical technique to address anatomic variants,” Dr. Najm says.
A new paper, published with colleagues at the Sydell and Arnold Miller Family Heart, Vascular & Thoracic and Cleveland Clinic Children’s, reports on outcomes for a total of 14 patients who have undergone the procedure.
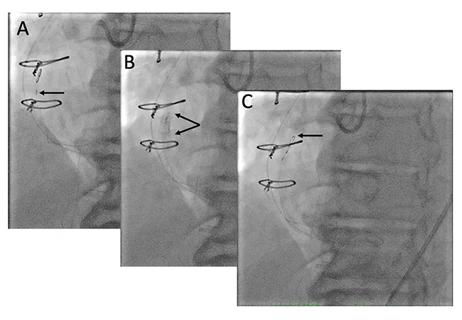
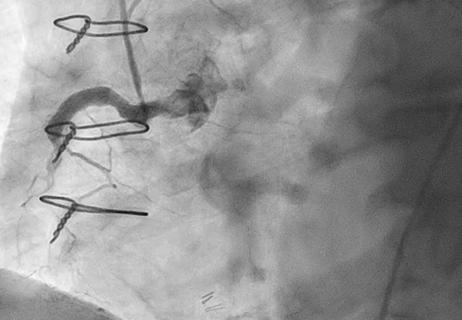
With a median of 11 months follow-up, all patients exhibited good anatomic outcome by computed tomography (CT) angiography before discharge. Postoperative index fractional flow reserve (iFFR) evaluation within three months of the procedure revealed absence of residual coronary compression in all patients who were tested preoperatively and improvement from preoperative values. All patients are now assigned to New York Heart Association functional class I, with excellent exercise tolerance.
Advertisement
Dr. Najm and colleagues offer four “surgical pearls” based on their experience thus far:
1) Management of the early takeoff of the left anterior descending artery (LAD). Five of the 14 patients in this series with AAOLCA and transeptal course had an “early takeoff” of the LAD from the left main coronary artery (LMCA), meaning that it arises and splits while still inside the muscle. In this situation, the unroofing becomes more complex because it must be started from the origin at the LMCA without sparing any sections of anterior myocardial bridging.
After the unroofing, the patch is tailored with a wider inferior wing. “You have to unroof it or you won’t get the right results. That’s why we’ve modified the patch shape that we put in to address that part,” Dr. Najm says.
2) Management of septal arteries. Septal arteries should be preserved throughout the unroofing and skeletonizing process. “We make sure they are unroofed and the patch is sutured to the muscle a few millimeters inferiorly, sparing all of these arteries. No septal arteries need to be sacrificed to achieve effective coronary decompression,” Dr. Najm says.
3) Management of minor superior branches to the pulmonary valve. Unlike septal arteries, the minor superior branches to the pulmonary valve aren’t critically important and can be sacrificed if necessary. However, they can often be preserved after successful unroofing by lifting the muscle bar below the pulmonary valve.
4) Dissector blades. When he began doing these procedures, Dr. Najm used a standard No. 15 blade for completing the coronary unroofing dissection following initial blunt division of the muscle overlying the artery with fine scissors. Now, he finds that a very fine Beaver blade knife works better by offering much greater precision. A No. 15 blade can still be used, though.
Advertisement
“A Beaver blade is one of the better ones for dissecting the muscle. And, I use it also to dissect the myocardial bridges, which are present in up to 40% of the patients,” Dr. Najm notes.
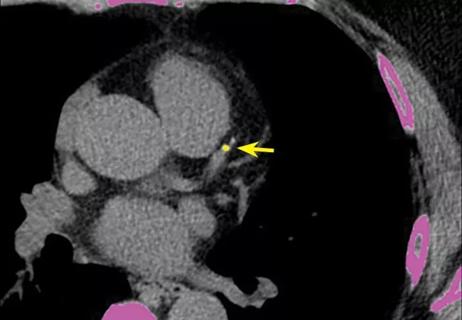
To evaluate patients who are either symptomatic or in whom an AAOLCA has been identified incidentally, Dr. Najm and colleagues advise preoperative multimodality provocative testing by one anatomic and two functional studies in both groups. CT has been the most useful modality for anatomic assessment of the coronary origin, course and surrounding structures or pathologic changes of the AAOLCA.
For functional testing, they recommend both noninvasive stress positron emission tomography and invasive intravascular ultrasound (IVUS) / iFFR for evaluation of ischemia (unless the patient child, in which case cardiac catheterization is used instead of IVUS/iFFR). Patients are selected for surgical repair if they have significant angina symptoms or abnormal preoperative study findings.
In addition, it’s crucial to preoperatively identify patients who have myocardial bridges apart from the transseptal segment of the AAOLCA, since their presence may perpetuate ischemia after the surgery.
Thus, Dr. Najm and colleagues advise performing both pre- and post-operative iFFR in all patients with transseptal AAOLCA course in order to evaluate the extent of any hemodynamically significant myocardial bridges, decide on the appropriate surgical plan, and gain objective evidence of ischemia resolution postoperatively.
Five more patients have undergone the Najm procedure since this report, in two cases by two other Cleveland Clinic surgeons under Najm’s supervision. “Every one of them has done well,” he says.
Advertisement
The team plans to publish again after the 30th patient and once some of the initial patients have achieved five years of follow-up.
Dr. Najm has received feedback from colleagues at other institutions informing him of their success with the procedure, and at least two others have published results with it. Some of the patients have been children, with equal success.
One problem: Najm has developed several surgical procedures for repairing anatomical heart defects, so which one is the “Najm Procedure?” His answer: “That’s for the surgical community to decide.”
Advertisement
Advertisement

Maintain a high index of clinical suspicion and consider the underlying etiology

5 biggest changes according to Cleveland Clinic experts
While procedural success rates lag overall, they shine for retrograde crossing
Lower success rates, more hospital MACE seen with poor-quality distal targets
Retrospective findings from an executive health program spur interest in broader studies
Growing awareness of impact leads to proliferation of procedures

A reliable and reproducible alternative to conventional reimplantation and coronary unroofing

Cleveland Clinic-pioneered repair technique restores a 61-year-old to energetic activity