Locations:

Recent breakthroughs have brought attention to a previously overlooked condition

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/39be7af6-51d0-4e68-8468-9f17ccdfa7d4/bronchiectasis-Inflection-point)
patient coughing
Bronchiectasis has been somewhat of an overlooked chronic pulmonary condition, in part due to its unique challenges related to multiple underlying causes. It is often misdiagnosed due to the wide variation in its causes and has historically had limited treatment options. Recently, however, there has been a renewed and transformational push towards more research and funding, which has led to the development of organizations and centers. Among these is the Bronchiectasis and NTM Association, which has pushed to have centers of excellence in every state where patients can get comprehensive care.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“About a year ago, we were selected to join the Bronchiectasis and NTM Care Center Network, which expands collaboration, increases visibility, and improves patient access to expert care,” says Anas Hadeh, MD, Director of the Pulmonary and Critical Care Medicine Fellowship Program at Cleveland Clinic in Florida. “We are currently the only center in the state of Florida that has a full care center. We also do research, quality improvement, patient education and staff education.”
Dr. Hadeh says renewed industry interest has also helped shine more light on the condition. With the FDA approval of the first treatment option for bronchiectasis (brensocatib), research has shifted away from antibiotic and infection treatment approaches toward inflammation treatments.
“The ASPEN study was a Phase 3 clinical trial that evaluated the efficacy and safety of brensocatib for treating non–cystic fibrosis bronchiectasis,” explains Dr. Hadeh. “Findings from this and other studies have shown that it is not the infection itself that primarily drives disease burden, but rather the underlying inflammation—particularly neutrophilic inflammation. Targeting this inflammatory pathway may help reduce exacerbations and improve outcomes for patients.”
He continues, “So, while physicians are getting more organized around bronchiectasis, the industry is also trying to bring therapeutics to our patients. It’s this perfect environment because we finally have new treatment options that we can implement in a multidisciplinary fashion to care for this disease.”
Advertisement
At Cleveland Clinic Florida, pulmonologists are primarily responsible for bronchiectasis care, but Dr. Hadeh notes that care is a collaborative effort. Pulmonologists work alongside infectious disease (ID) experts, microbiologists, respiratory therapists, gastroenterologists, nutritionists, pharmacists, thoracic surgeons, ophthalmologists and audiologists.
“This is something that is quite novel to have an infectious disease and a pulmonologist meet with a patient together,” says Dr. Hadeh. “Previously, we would have patients who traveled from all over the state to come and see an infectious disease physician on one day. Then they go home, and they have to come back and see the pulmonologist another day and keep going back and forth. We established our current model of care to help streamline everything — the patient meets with all their specialists on the same day, so it reduces time and travel for our patients, and helps strengthen communication on the provider side as well.”
In this model, patients are brought in by a nurse coordinator and meet with fellows and trainees during rounds to collect their history and vitals.
“The fellows come back and present to the pulmonologist and ID,” says Dr. Hadeh. “So, this is another layer to the model where our fellows are engaged in the process, and they get all this training and exposure to bronchiectasis care. We’ll discuss the patient’s scans and cultures, and we come together as a group right then and there to determine the best course of treatment, and patients love that. There’s no more, ‘Let’s wait to see what the infectious disease specialist or the GI specialist has to say at your next appointment.’ We also have something similar to a tumor board where we all meet once a month to discuss individual patients.”
Advertisement
In addition to the focus on elevating care, there is also heavy prioritization on research. Currently, two clinical trials are in process. One trial, the MannKind Clofazimine Inhaled Study, is actively enrolling, which looks at inhaled clofazamine for refractory mycobacterium avium complex (MAC) patients. Dr. Hadeh also notes that Cleveland Clinic Florida will soon be a site for the AIRTIVITY trial, and another trial that looks at inhaled immunoglobulin administration for patients with bronchiectasis.
Beyond these industry-funded trials, the Bronchiectasis Center at Cleveland Clinic is also involved in a few internally-funded trials.
“One of our studies is exploring the incidence of nontuberculous mycobacteria(NTM)infection in a lung cancer screening program,” says Dr. Hadeh. “In other words, you have patients who are going for bronchoscopies for suspected lung cancer, and we're trying to report the incidence and the prevalence of misdiagnosed cancer that is actually an NTM infection.”
Dr. Hadeh mentions another study he’s involved with that is looking at the effect of cognitive behavioral therapy on NTM treatment adherence. NTM treatments often come with a lot of side effects, so cognitive behavior therapy could allow those patients to stick with the treatment longer. If patients complete the treatment, the cure and conversion rates of their sputum are going to be higher.
“This is really an exciting time in bronchiectasis treatment,” says Dr. Hadeh. “We’re really at this inflection point where treatment and industry interest are increasing while providers are organizing themselves and sharing insights and establishing best practices. At Cleveland Clinic, we’ve been very pleased with the response to our multidisciplinary approach to care, and we’re also very excited about what’s on the horizon in terms of bronchiectasis care and research.”
Advertisement
Advertisement

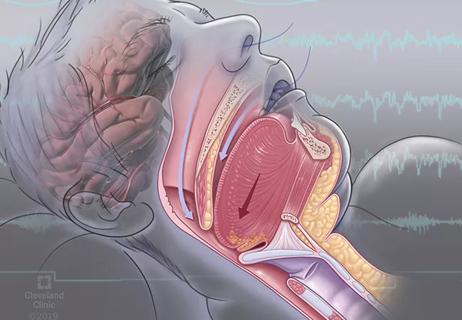
A look at the emerging link between intermittent hypoxia and broader health effects in COPD

Case study illustrates the potential of a dual-subspecialist approach

Findings show profound muscle loss variance between men and women
New tools and protocols to improve care

Endoscopic balloon dilation during pregnancy helps optimize outcomes
For the first time, risk is shown after accounting for underlying contributions of pulmonary disease

Surgery is typically the only option for the most severe cases, but a minimally invasive procedure is reducing morbidity and recovery time for patients

First five-year prospective study provides valuable data to guide decision-making