Locations:

Excellent results achieved using internal cantholysis on coloboma
Large eyelid defects such as colobomas in newborns can be difficult to treat for a variety of reasons, notably the lack of excess lid tissue available for grafting and the increased risk of amblyopia.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
While delaying treatment until a child is about 3 or 4 years old is generally preferred, some cases cannot wait due to the risk of exposure keratopathy.
In a case study that illustrates this dilemma, published in theDigital Journal of Ophthalmology last year, a 5-day-old girl, born at full term, presented to the Cleveland Clinic Cole Eye Institute for evaluation of right eyelid irregularities.
On initial examination, the eye was found to have a preauricular skin appendage, a small temporal limbal dermoid and coloboma that involved about 75 percent of the upper lid. Visual acuity was determined to be light perception in both eyes but there was near total exposure of the right corneal surface, with trace inferior punctate epithelial erosions. No epithelial defect was found.
Aggressive surface lubrication was prescribed. At 2 weeks’ follow-up, the baby was found to have developed a small right inferior corneal ulcer. Topical antibiotics were begun, and the patient was scheduled for surgical repair, says Julian D. Perry, MD, Head of Oculoplastics at Cole Eye Institute, and a co-author on the paper.
Although most routine preoperative testing (including blood work, newborn metabolic screening, chromosomal microarray analysis and hearing screen) were unremarkable, a moderate secundum atrial septal defect with mild dilation of the right ventricle was revealed by echocardiography. X-ray of the chest and abdomen showed thoracic vertebral and left rib segmentation anomalies.
Although most colobomas are idiopathic, isolated findings, the Cole Eye Institute oculoplastics team felt that the clinical findings in this case warranted a presumptive diagnosis of Goldenhar syndrome. This is a condition in which a child is born with irregular development of the eye, ear or spine. Facial asymmetry is common, along with benign growths on the eyelids and malformed or absent ears. The heart, lungs, kidneys and central nervous system can also be affected.
Advertisement
The incidence of Goldenhar is estimated to be one case in every 3,500 to 25,000 births. The cause is unknown. Treatment varies based on symptoms and their developmental consequences.
Since this condition can be linked to increased risk of adverse reactions to anesthesia, and this patient had cardiac involvement, a less invasive surgery that allowed quicker operative time was appealing, Dr. Perry says.
“Our surgical options included sliding tarsoconjunctival/myocutaneous flaps, skin grafts or large lateral myocutaneous flaps,” Dr. Perry explains. “We opted to use internal cantholysis followed by direct closure to repair the large upper lid coloboma.”
This approach (see figure below) does not require supplementary sutures, and produces excellent cosmetic and functional results, important considerations for such a young patient, he says. It also is easily converted into a semicircular flap intraoperatively if recruited tissue is inadequate to allow for wound closure.
When the sutures were removed three weeks after surgery, the child had excellent eyelid movement and contour. At nine months’ follow-up, there was a favorable eyelid contour with mild ptosis and lagophthalmos, but vision was not impacted. There was persistence of superomedial periorbital hollowing because the severe coloboma also involved the super superomedial fatty tissues in addition to the full thickness of the eyelid
Dr. Perry says the child’s eyelid should develop normally without the need for further surgery. The eyelid defect that extended into the orbit can be addressed cosmetically as the patient ages, as she desires.
Advertisement
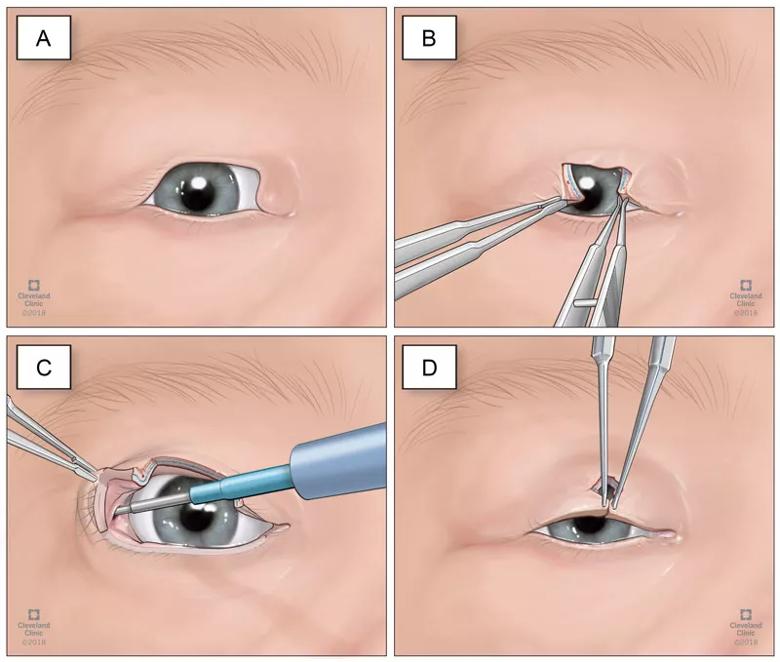
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/5c822798-2414-4f08-aa75-6139a94817d4/18-EYE-4077-Perry-CQD-Inset_jpg)
A, Large upper eyelid coloboma. B, Edges of the defect are freshened with #15 blade and an initial attempt at direct approxi-mation failed to close the defect. C, The conjunctiva is incised approximately 3 mm superior to the tarsus in the right upper eyelid lateral fornix, and the superior crux of the lateral canthal tendon is lysed with a monopolar cautery instrument. D, The wound edges are precisely anastomosed without undue tension.
Advertisement
Advertisement

The drug does not provide lasting disease control for most patients

New service for patients with diabetes will make annual screening more convenient

Gonioscopy can help determine next steps in reducing IOP

Similarly, patients with noninfectious uveitis have a higher risk of being diagnosed with an autoimmune disease within five years

A review of pathophysiology, risk factors, clinical presentation and treatment options

How computational tools and personalized biomechanics can improve keratoconus detection, ectasia risk assessment and surgical outcomes

Motion-tracking Brillouin microscopy pinpoints corneal weakness in the anterior stroma

Registry data highlight visual gains in patients with legal blindness