Locations:

Innovative construct restores function after resection of softball-size chondrosarcoma

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/07b33a79-edd9-48cf-89e5-911e2e8761d7/22-ORI-2662859-CQD-650x450b_jpg)
22-ORI-2662859 CQD 650x450b
By Nathan Mesko, MD, and Daniel Raymond, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 59-year-old patient presented with a 14-centimeter tumor on his sternum. He noticed the lump after a motor vehicle accident 13 years earlier. Over the years he had been told that the lesion was benign, but it had continued to grow larger than the size of a softball. CT imaging of the tumor detected characteristics of a bone lesion containing cartilage, a concerning finding in an adult, whose growth plates have long been closed. Needle biopsy revealed a chondrosarcoma diagnosis.
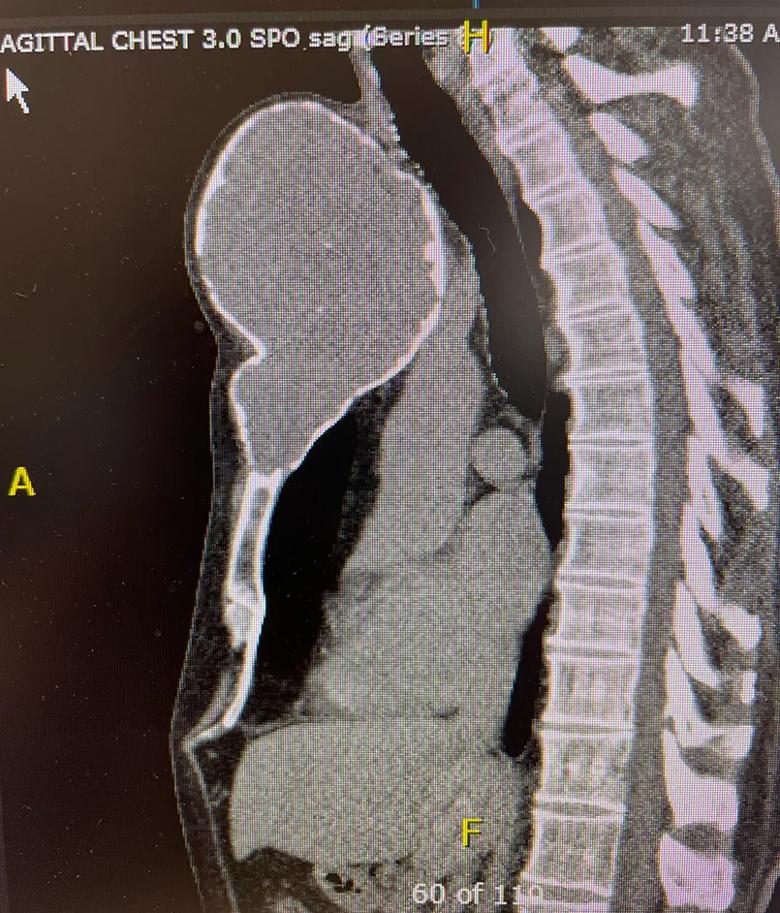
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9ae0b5d4-5ed3-4369-9b52-770318131d65/22-ORI-2662859-CQD-Inset-2_jpg)
CT imaging showed a cartilage tumor expanding the sternum, suspicious for a chondrosarcoma. This was later proven following a biopsy procedure.
Chondrosarcoma is the most common bone sarcoma in adults and the third most common bone sarcoma in humans, after osteosarcoma and Ewing sarcoma, which are more prevalent in younger populations. There is a spectrum of chondrosarcoma subtypes, some indolent (like this case) and some aggressive. More aggressive subtypes have significant prognostic implications, with survival lasting potentially just a few months. Chondrosarcoma tumors rarely respond to chemotherapy or radiation therapy, so treatment typically is resection alone.
Even if the tumor in this case had been benign, it still would have required resection as it had begun to compress the trachea, the esophagus and the left carotid artery.
The tumor did not appear to involve deeper thoracic structures, however its removal would be a formidable challenge. Along with most of the sternum, both sternoclavicular joints — the only skeletal attachment between the arms and axial skeleton — would need to be resected and then reconstructed.
Reconstructing the sternum is critical for protecting the heart and other thoracic organs, for recreating anterior support for the spine (to prevent kyphosis) and for providing an anchor for arm mobility. However, because removal of the sternum and sternoclavicular joints is so rare, reconstruction requires a novel approach that balances the need for stable fixation with allowances for subtle motion. There are only limited descriptions of this type of reconstruction in medical literature. There is no established standard of care, and artificial implants do not exist.
Advertisement
Typical reconstruction techniques using plates and screws or other fixation devices are not appropriate for sternoclavicular anatomy as this anatomic location must accommodate motion when arms are moved or lifted, or when breathing expands and contracts the chest. In this case, the challenge was to recreate chest wall anatomy while permitting mobility.
Thoracic and orthopaedic surgeons collaborated to design a new construct using a cadaveric femur in place of a sternum. The femur would be suspended from both clavicles using a combination of technologies including a synthetic aortograft (a flexible but tough polyethylene tube used to treat aortic aneurysms), polyethylene terephthalatesuture and Syndesmosis TightRope® (Arthrex) fixation (a polyethylene cord used for ankle stabilization).
Before the construct could be built and the surgical procedure attempted, an appropriately sized femur would be obtained from a bone bank.
During the procedure, the thoracic surgeon removed the tumor and sternum while the orthopaedic surgeon fashioned the new construct. The cadaveric femur was anchored to the remaining sternum via a scarf joint, secured with sutures. To build the sternoclavicular joints, the TightRope fixation devices first were placed to anchor the sternum to the clavicles. The aortograft, which had been affixed to the femur with cables, was wound around the cut ends of the clavicles and anchored with additional cables. Finally, polyester sutures were woven between the clavicles by means of a cannulated screw in the femur. The construct was covered with mesh, which would prevent lung herniation in the small lateral defects as well as provide an additional layer of support.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2834906c-51b0-4f40-95a6-1a119de274b5/22-ORI-2662859-CQD-Inset-3_jpg)
A femoral allograft was obtained from a national bone bank and prepared to fit the sternal defect.
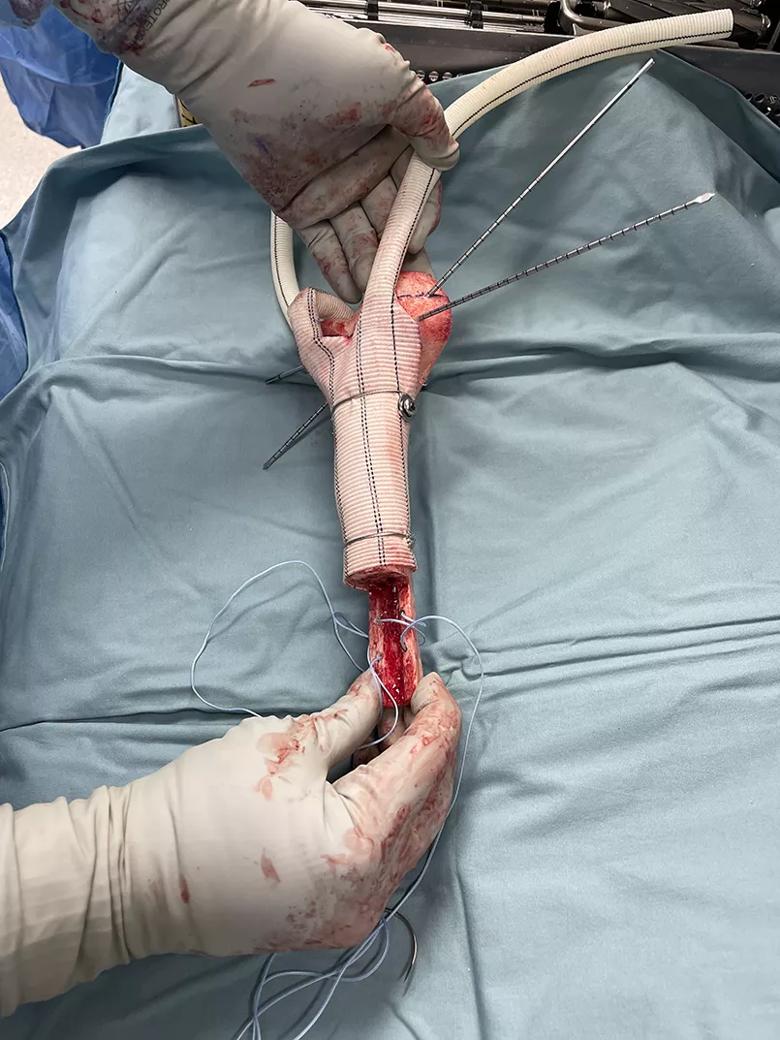
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c2490ea8-50dc-4671-acff-8e456103be9d/22-ORI-2662859-CQD-Inset-4_jpg)
After the femoral allograft was fashioned to planned specifications, it was overwrapped with a synthetic aortic graft and fixated with a combination of cables, cannulated screws, ultrahigh-molecular-weight polyethylene core suture and polyethylene terephthalate tape.
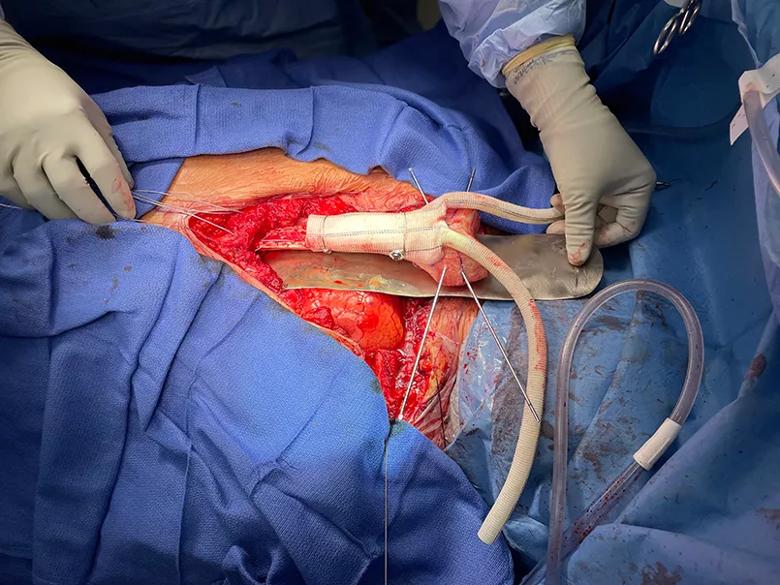
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/09aadc0c-7928-4c39-abd1-bfae0a99b950/22-ORI-2662859-CQD-Inset-5_jpg)
The reconstructed allograft implant was inserted into the sternal defect, using the scarf joint to slide under the remaining lower (distal) part of the native sternum bone.
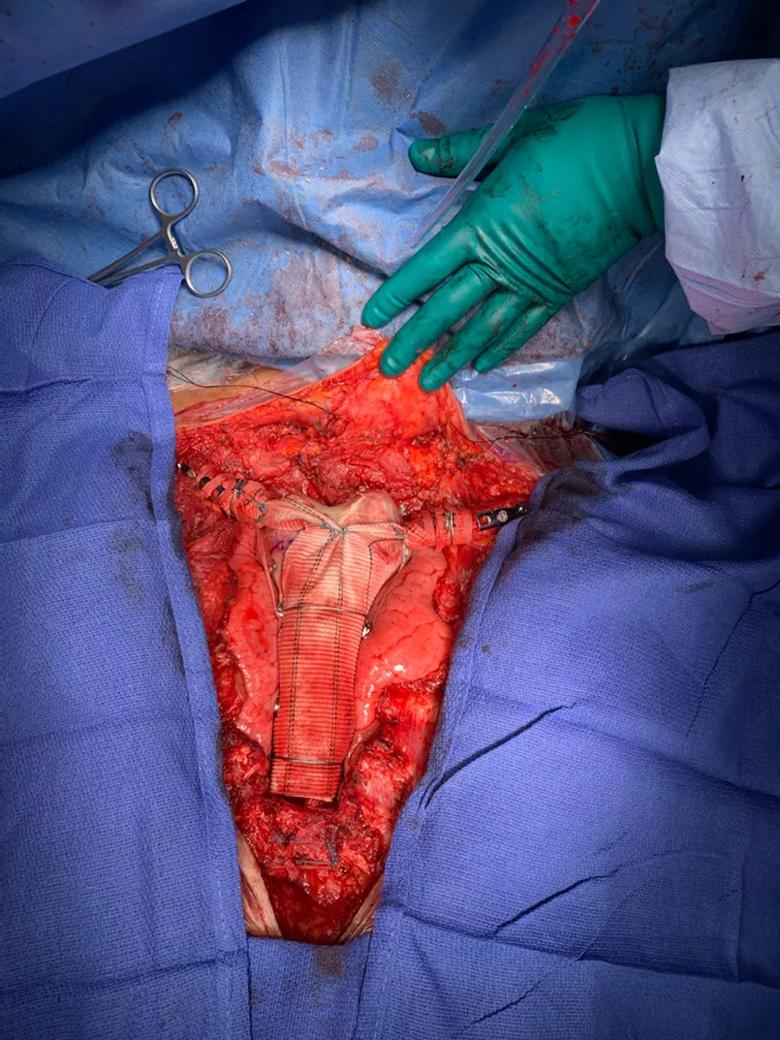
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ec0d32e1-13ae-4c98-af81-1c8400a2a3b1/22-ORI-2662859-CQD-Inset-6_jpg)
The completed reconstruction was suspended between the clavicles using a suspensory technique involving a mechanism normally used for fixing ankle fractures and high ankle sprains. The aortograft material was wrapped around the clavicles and further supplemented with polyethylene terephthalate tape suspension.
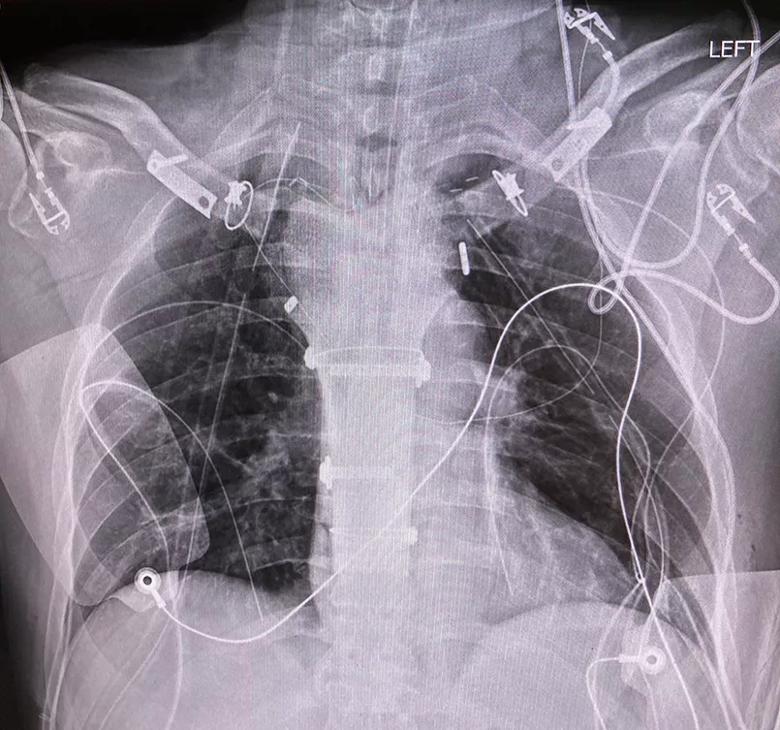
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7d4a81f2-658a-4555-8224-d2b8f4ac1663/22-ORI-2662859-CQD-Inset-7_jpg)
A chest X-ray shows the final sternal reconstruction.
Three months after surgery, the patient is pain-free and back to work. He has been advised to avoid heavy lifting. He will be followed closely and watched for scoliosis and any change that may affect the construct, especially once he is able to lift his arms above 90 degrees. Scar tissue will further anchor the construct.
Due to the clean resection of the chondrosarcoma, the patient is expected to have a normal life span. For chondrosarcoma in general, survival is 70-75% at five years. With nonaggressive chondrosarcoma, as in this case, survival can be 99% at five years.
This case highlights a novel approach to reconstructing a challenging anatomic site. Existing alternatives, such as 3D-printed anatomy and other custom-built implants, would require a lengthy approval process not preferable for a patient with cancer. In addition, even custom implants cannot readily solve the dilemma of balancing the need for motion with durable fixation and reconstruction. The cadaveric femur construct, incorporating an aortograft and ankle-fixation mechanism, leverages technologies readily available and provides durable fixation with robust materials while allowing for motion as needed.
The construct also showcases the synergy of skill sets required to develop innovative solutions for challenging cases. In this case, the collaboration of thoracic and orthopaedic surgery experts led to a unique approach — combining a cadaver bone, cardiovascular technology and an ankle suspension mechanism — that never would have evolved without multidisciplinary teamwork.
Advertisement
Dr. Mesko is Center Director, Orthopaedic Oncology, and co-Director of Sarcoma Care at Cleveland Clinic. Dr. Raymond is a thoracic surgeon in the Sydell and Arnold Miller Family Heart, Vascular & Thoracic Institute at Cleveland Clinic.
Advertisement
Advertisement

Personalized reconstruction is an alternative to leg amputation or flail limb

Soft tissue pathologist discusses research into incorporating genomic data to improve risk stratification

Machine learning models assess intraoperative tissue perfusion
Previous studies, trial aims and the potential role of immunotherapy

A snapshot of key stats from one of the world's busiest centers

Join us in Cleveland July 17 for a practical, first-of-kind course

Case study of radial-to-axillary nerve transfer for tumor-related deltoid nerve injury

Study also finds that 26% of children with cancer have mutations in DNA repair genes