Locations:

Podcast content: This podcast is available to listen to online.
Listen to podcast online (https://www.buzzsprout.com/2250706/18476269)
Lymphangioleiomyomatosis (LAM) is a rare and progressive cystic lung disease primarily affecting women of childbearing age. It is characterized by the infiltration of the lung parenchyma by abnormal, smooth muscle-like cells and epithelioid cells known as LAM cells or LAM lesions. It leads to the destruction of lung tissue and the formation of lung cysts.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“LAM was previously considered an interstitial lung disease, but with increased knowledge and discoveries showing multi-system involvement and the presence of LAM cells in blood and lymphatics, a genetic component, there are reports of LAM lesions or LAM cells recurring in transplanted lungs,” says Joy Ussavarungsi, MD, Head of the Rare Lung Disease Clinic at Cleveland Clinic, in a recent episode of Respiratory Exchange. “So, it is now recognized as a low-grade metastatic neoplasm.”
In the podcast episode, Dr. Ussavarungsi, and Les Tolle, MD, Section Head for Diffuse Parenchymal Lung Disease at Cleveland Clinic, share valuable insights into LAM’s pathophysiology, diagnosis, clinical presentation and treatment options, including the transformative impact of mTOR inhibitors like sirolimus.
“In the past, when LAM was diagnosed, it was considered fatal without a lung transplant, but today, the median survival for patients is estimated to be over 20 years after diagnosis,” explains Dr. Ussavrungsi. “The data say that transplant-free survival probability is more than 90% at five years, so patients now have much better outcomes. We also believe that sirolimus or everolimus, both of which are mTOR inhibitors, can significantly improve the survival rate for LAM patients.”
Click the podcast player above to listen to the episode now, or read on for a short, edited excerpt. Check out more Respiratory Exchange episodes at https://my.clevelandclinic.org/podcasts/respiratory-exchange or wherever you get your podcasts.
Advertisement
Dr. Les Tolle: You mentioned that there are two types, genetic and sporadic cases. So, can you talk a little bit about how these patients present? Do the two types present differently? Are they similar? What are the demographics of these patients? And speaking as a pulmonologist, what are the things that we have to look out for from a pulmonary perspective from these patients?
Dr. Joy Ussavarungsi: So, LAM mostly affects women of childbearing age, and the estimated prevalence is around three to seven per million women worldwide. But this number is likely underestimated now as awareness grows and diagnostic capabilities improve. And most LAM patients, usually sporadic LAMs, are diagnosed in their third or fourth decade of life, and most of them are premenopausal women.
However, the conditions can affect individuals from pre-adolescents to the elderly. When talking about [tuberous sclerosis complex] TSC-LAM, lung cysts consistent with LAM are present in about half of women with TSC and in only around 10% of men. We may detect more LAM cases because international TSC guidelines have recommended CT screening for LAM in women with TSC starting at the age of 18.
If we’re talking about symptoms for LAM, pulmonary manifestations are the most common presentation because they often present with shortness of breath, which can be progressive or pneumothorax.
In addition to this, LAM patients can present with extra-pulmonary features, such as an abdominal mass. A common one is a benign tumor known as angiomyolipomas, or AMLs, which are commonly found in the kidneys. But another unique feature is a lymphatic involvement, as we know that the lymph cells can spread through the lymphatic system. So, this may present as a lymphadenopathy colors effusion, either pleural effusions or ascites and lymphatic mass called lymphangioleiomyomas, typically found in the abdominal, pelvic or retroperitoneal areas.
Advertisement
Dr. Les Tolle: That's super interesting. One of the things I actually had a question about is when I learned about LAM, we thought of it as an exclusively female disease, and you mentioned that even men can have LAM. Can you talk a little bit more about that, or is it just pretty unknown in its sporadic, rare cases?
Dr. Joy Ussavarungsi: There is also a thought that hormonal influences seem to play a role in the LAM disease and LAM progression and as you said, this disease predominantly affects women.LAM cells also express estrogen and progesterone receptors. So sometimes this severity often worsens with estrogen supplementation or during pregnancy. Additionally, from LAM repository data, the rate of lung function decline can slow down after menopause, which further supports the role of estrogen in this disease.
Dr. Les Tolle: I just had a sort of a separate question about that. So now I have someone who's generally a younger woman in my clinic, whom I'm suspicious of LAM. How do I make a formal diagnosis of LAM? What, what am I looking for in terms of imaging, spirometry, tissue diagnosis, all those things?
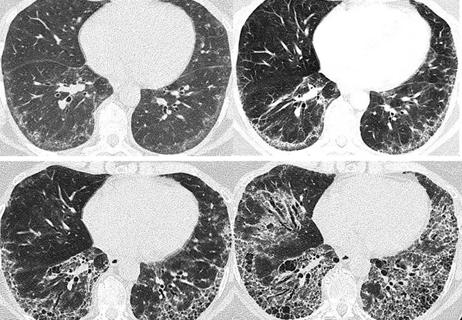
Dr. Joy Ussavarungsi: CT plays a major role in diagnosing LAM. Usually, the CT will show a round, uniform, thin-wall cyst, usually distributed in both lungs, and usually, we will see normal lung tissue in between. But keep in mind, many conditions can mimic LAM.
For example, lymphoid interstitial pneumonia or LIP in autoimmune disease, especially Sjogren's syndrome is one of the genetic conditions that can cause a scattered lung cyst with skin lesions or kidney tumor. Sometimes it's confused with ultra-rare lung categories, like amyloidosis or light chain deposition disease, which can also cause scattered lung cysts. So, we cannot rely solely on CT for a LEM diagnosis. In addition to this imaging, fortunately, LEM also has a serum biomarker called vascular endothelial growth factor D or VFD.
Advertisement
If the level is above 800, LAM can be diagnosed confidently without a biopsy. And nowadays, we can diagnose LAM with a thorough evaluation without the need for a biopsy.
For example, if the patient presents with characteristic CT findings, we need to try to look for one or more of the supporting features. For example, [these could include] the presence of tuberous sclerosis complex, AML lesions, lymphatic mass, lymphangioma lesions, colored effusions from pleural effusions orascites and elevated serum FD level.
In cases with atypical CT findings or when supporting features of LAM are absent, yes, a biopsy may be considered. But personally, the decision to proceed should carefully balance the potential benefits of a definitive diagnosis in guiding or changing management with the risk of the possible complications.
For example, if our patients have no symptoms or only a few cysts or very mild disease burden, a probable clinical diagnosis of LAM with serial monitoring is reasonable, especially if the pathology will not change our management at this time. But when tissue sampling is deemed necessary, LAM guidelines recommend considering transbronchial biopsy first before proceeding with a surgical biopsy. In my opinion, cryobiopsy can, can be considered to increase the yield, but the decision will depend on the center's expertise.
Advertisement
Advertisement

Overexposure to the common alloy can lead to an autoimmune response called sensitization

A review of treatment options for patients who may not qualify for surgery

Rising rates in young miners illustrate the need for consistent prevention messaging from employers and clinicians

Multidisciplinary focus on an often underdiagnosed and ineffectively treated pulmonary disease

Management and diagnostic insights from an infectious disease specialist and a pulmonary specialist

Treatments can be effective, but timely diagnosis is key

A Cleveland Clinic pulmonologist highlights several factors to be aware of when treating patients
Patient experience improves with a multidisciplinary approach