Locations:

Understanding VC anatomy is critical for transcatheter tricuspid valve interventions

Dimensions of the superior and inferior venae cavae (VC) at various levels are larger for patients with isolated severe tricuspid regurgitation (TR) compared with patients who have isolated mitral regurgitation (MR) or no valvular dysfunction. However, specific dimensions do not vary substantially in individuals throughout the cardiac cycle.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Cleveland Clinic researchers reached these conclusions after measuring VC anatomic dimensions using multiphase cardiac CT. Details of their study were discussed in a poster presentation at the 2023 scientific session of the American College of Cardiology.
“Knowing the dimensions of the venae cavae and their spatial relations to the tricuspid valve (TV) in the setting of severe TR has important implications for caval valve implantation devices, including sizing, delivery and anchoring,” explains Cleveland Clinic resident Osamah Badwan, MD, who presented the study.
Transcatheter TV interventions are increasingly being developed and used to address severe TR in patients for whom surgery is too risky. Designed to prevent downstream complications of reflux, the devices either target the VC or use the VC for access while targeting the TV directly.
Devices for caval valve implantation must be sized correctly, but little is known about VC dimensions either normally or in the setting of severe TR. These transcatheter procedures can also be challenging because VC anatomy can vary with respect to angulation, distance and offset between the VC axes and the TV axis.
To address this lack of knowledge of VC anatomy, the Cleveland Clinic investigators sought to characterize important anatomic characteristics of the VC as well as spatial relationships between the VC and TV in severe TR, using patients without valve dysfunction and age-matched patients with severe isolated MR as comparison groups.
Advertisement
Three study cohorts were drawn from patients who had undergone multiphase cardiac CT with right-sided contrast at Cleveland Clinic between 2017 and 2022. They consisted of:
Multiple dimensions were compared, including measurements of key areas in systole and diastole. All measurements were indexed to body surface area.
Results included the following (see Figure):
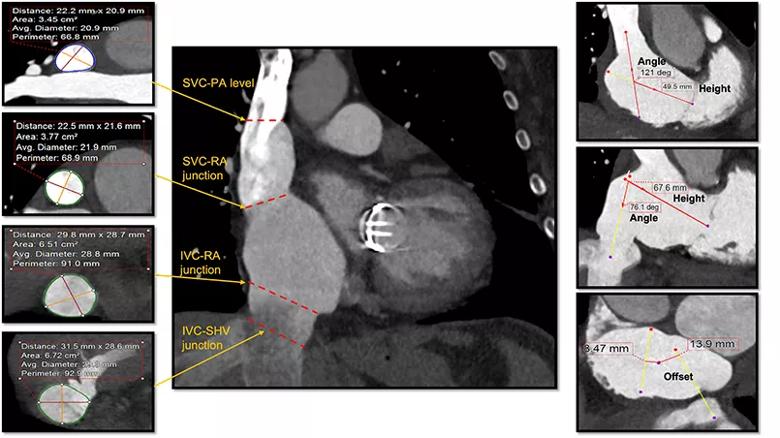
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7c782069-3656-41f9-b71a-b9b9ab0de612/23-HVI-3606663-CQD-Inset_jpg)
Figure. Cardiac CT measurements of venae cavae dimensions at various levels. IVC = inferior vena cava; RA = right atrium; SHV = suprahepatic veins; SVC = superior vena cava; PA = pulmonary artery.
Co-investigator Samir Kapadia, MD, Chair of Cardiovascular Medicine at Cleveland Clinic, highlights key findings of the study and their implications:
Advertisement
Cleveland Clinic interventional cardiologist Rishi Puri, MD, PhD, another investigator in this study, points out that much innovation is taking place in the TV landscape, with repair, replacement and coaptation embodiments currently being tested at various stages of development.
“As some of these large-bore delivery systems undergo human trials, we have come to appreciate that how they are positioned at vena cava entry significantly affects one’s ability to orient in a coaxial manner to the tricuspid valve,” he says. “Understanding coaxiality is fundamental to optimizing many transcatheter TV device deployments, and this study’s data inform that.”
An overview of caval valve implantation therapies was published by Dr. Puri and European colleagues in the Journal of Clinical Medicine (2021;10:[19]:4601). Details of the TricValve® Transcatheter Bicaval Valves System were described in a previous Consult QD post. Testing of that system versus standard medical therapy in a pivotal randomized clinical trial is underway, with Drs. Kapadia and Puri as principal investigators under the coordination of the Cleveland Clinic Coordinating Center for Clinical Research (C5Research).
Dr. Badwan adds that the study detailing VC anatomic characteristics in severe TR is expected to be published as a full-length article soon.
Advertisement
Advertisement

Study supports addressing mitral regurgitation before mild tricuspid regurgitation progresses

TRISCEND II trial reports 1-year results

Limited data and experience will translate to a cautious rollout
Cleveland Clinic study argues against waiting for symptoms to develop
TEER is found to be a safe and good option for severe TR in select patients

Cleveland Clinic report shares details and outcomes of novel technique for open repair

Join us in New York Dec. 6-7 for broadened version of a CME crowd-pleaser
Investigators conclude that improved self-reports go beyond possible placebo effect for severe TR