Locations:

First-ever transcarotid artery revascularization trial with no strokes or device-related deaths

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/bec65021-7aea-4d83-bb23-28b9d0289323/carotid-artery-bifurcation-cqd)
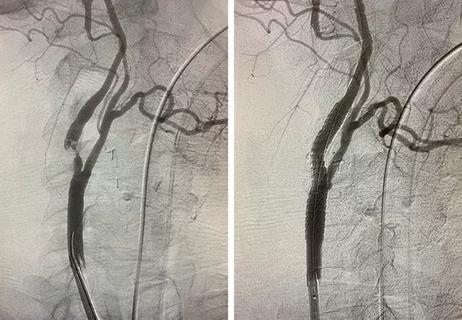
scan showing a blockage in an artery in the brain
A new transcarotid approach to carotid disease that combines flow reversal with an integrated embolic protective filter achieved a major adverse event rate of only 0.7% at 30 days with no strokes, neurological deaths or cranial nerve injuries in a population at high surgical risk.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
That’s according to the pivotal PERFORMANCE III trial, a prospective multicenter study evaluating transcarotid artery revascularization with integrated embolic protection (TCAR-IEP) using the investigational Neuroguard IEP® Direct System (Contego Medical). Thirty-day outcomes of the trial, led by Sean Lyden, MD, Chair of Vascular Surgery at Cleveland Clinic, were recently published in the Journal of Vascular Surgery.
“It’s the first trial since the development of TCAR technology to report no strokes and no device-related deaths,” says Dr. Lyden. “It has many clinicians excited that we are further moving the needle on the safety of this procedure compared with surgery.”
TCAR has become established as an alternative to carotid endarterectomy (CEA) and transfemoral carotid artery stenting, as it offers less invasiveness than CEA and lower neurological event rates compared with transfemoral stenting. That may be due in part to TCAR’s temporary reversal of blood flow from the intracerebral circulation through the device sheath, which captures embolic debris released during the stenting procedure.
Questions have remained, however, about whether carotid flow reversal alone provides sufficient cerebral protection. A potential concern is retrograde collateral flow from the external carotid artery, which is not excluded from the cerebral circulation during TCAR as it is in CEA.
“When we do transfemoral carotid stenting, minor strokes have been a cause for concern,” Dr. Lyden says. “Some of the minor stroke risk may be due to the size mismatch between procedural debris and available filters.” He notes that studies have shown that a large share of particles dislodged during carotid stenting are smaller than 100 microns, but standard distal filters and mesh-covered stents have larger pore sizes that let such particles pass through. Previous data from the PERFORMANCE II trial in patients undergoing transfemoral carotid stenting showed improved outcomes relative to historical controls with the addition of an integrated embolic filter to the stent.
Advertisement
These concerns and observations informed the design of the TCAR system studied in PERFORMANCE III. The Neuroguard IEP Direct System is a three-in-one platform containing a self-expanding nitinol stent, a prepositioned semi-compliant post-dilation balloon and an embolic protection filter with 40-micron pores. The platform is housed on a 70-cm catheter designed for the shorter working distance of a direct carotid access approach. “A 40-micron filter was integrated into the system to capture debris that wouldn’t be caught in a TCAR case done with the commercially available ENROUTE™ Transcarotid Neuroprotection System [Boston Scientific], adding a second layer of protection,” Dr. Lyden notes.
Additionally, the system eliminates the femoral venous access required by the ENROUTE System; instead, blood is drained by gravity into a collection bag positioned 20 cm below the carotid access site, with the differential between the patient’s arterial pressure and atmospheric pressure driving the flow reversal.
“No arteriovenous shunt is required,” Dr. Lyden explains. “The thinking was, why not let the blood drain into a bag and then be discarded? It’s going to be similar to the amount of blood lost with either CEA or transfemoral carotid artery stenting.”
The PERFORMANCE III investigators enrolled 178 patients across 26 U.S. centers and one site in France. Thirty-two patients completed a lead-in cohort that served to establish proficiency in the procedure. The remaining 146 patients made up the pivotal cohort for the primary analysis.
Advertisement
Eligibility required symptomatic stenosis ≥ 50% or asymptomatic stenosis ≥ 70% in the internal carotid artery or at the carotid bifurcation. Case complexity was generally high, as almost all patients had lesions that were moderately to severely calcified, mean stenosis was 82% and more than two-thirds of patients had high-risk physiological features.
The primary end point was a composite of major adverse events — specifically, stroke, myocardial infarction (MI) or death — at 30 days after intervention. Results were benchmarked against a prespecified performance goal of 11% that was based on six earlier carotid stent IDE trials.
In the intention-to-treat analysis of the 145 patients with 30-day follow-up, the composite end point occurred in one patient (0.7%; 95% CI, 0.02%-3.78%). This single event, a cardiac death 18 days after the index procedure, was adjudicated as unlikely to be procedure-associated and unrelated to the Neuroguard IEP Direct device. There were no strokes of any kind (major, minor or ipsilateral) and no neurological deaths.
The 3.78% upper bound of the 95% confidence interval for the composite of major adverse events was well below the study’s prespecified performance goal of 11% (P < .001). Notably, in the study’s secondary per-protocol analysis of 144 patients, the composite event rate was 0% because the patient with cardiac death at 18 days had had a prior MI within 30 days before the TCAR procedure, thereby violating the protocol.
Outcomes on other secondary end points included high rates of acute, technical and procedural success (98.6% to 99.3% for all), no need for blood transfusions, and an absence of any cranial nerve injuries or stent thromboses.
Advertisement
Mean flow reversal time in PERFORMANCE III was 7.4 minutes, shorter than the 12.9 and 11.0 minutes in the ROADSTER and ROADSTER 2 pivotal trials of the ENROUTE system for TCAR. While noting that cross-study comparisons are inherently limited, the PERFORMANCE III investigators point out in their study report that Vascular Quality Initiative registry data show that stroke risk in TCAR climbs by 2.7% with each additional minute of flow reversal beyond five minutes. Notably, reversal durations beyond 10 minutes are associated with a 38% rise in stroke risk.
“Ten minutes seems to be the sweet spot,” Dr. Lyden says. “If you’re under 10 minutes, your outcomes are fantastic. If reversal time goes above 10 minutes, stroke risk starts growing exponentially. So if a trial achieves a 7.4-minute reversal time early in the learning curve like this, people are going to be very interested.”
He attributes the efficiency gains to the TCAR-IEP technology’s design. By incorporating the post-dilation balloon within the stent delivery platform and eliminating femoral venous access, the system removes several procedural steps. “It eliminates four to five minutes from the procedure, on average,” Dr. Lyden says.
The PERFORMANCE III data have been submitted to the FDA, with potential commercial approval of this Neuroguard IEP Direct technology in the balance. “That could reshape the landscape of carotid intervention for patients at high risk for carotid surgery,” Dr. Lyden notes.
If approved, this new system would be the second TCAR system commercially available in the U.S., following the ENROUTE system’s 2015 clearance. A third TCAR device, a version of Inspire MD’s CGuard® system designed for direct carotid access, is also in late-stage clinical development. It addresses embolic risk through a dual-layer micromesh stent designed to prevent plaque extrusion rather than with a separate filter.
Advertisement
For now, Dr. Lyden says that the zero-stroke results with the TCAR IEP system in PERFORMANCE III require further validation, given the trial’s modest size. “A registry will be needed to show whether these results are scalable and whether this approach is as strong as we suspect,” he observes.
Meanwhile, his Cleveland Clinic colleague Ravi Ambani, MD, MBA, notes that the system offers promising practical attributes. “After being involved in several cases in both the PERFORMANCE III and ROADSTER 2 trials, I can attest that the Neuroguard IEP device is unique as well as easy to use and adopt in your practice,” says Dr. Ambani, a staff vascular surgeon. “It allows you to minimize procedural steps with the key components of filter, stent and balloon all integrated into one device. The prospect that we may have an approved device with zero strokes or device-related deaths in a pivotal trial is a first for our field. It promises to push the safety profile of TCAR forward in our ongoing efforts to improve patient outcomes.”
PERFORMANCE III was sponsored by Contego Medical. Dr. Lyden reports that he is a consultant for, and has performed research studies for, Contego Medical and other medical device companies.
Advertisement
A look at where TCAR and transfemoral carotid stenting are likely headed

JACC review calls for CMS to update coverage decision

Insights from the Cleveland Clinic experience and a multispecialty alliance

Insights on common questions from referring providers

A snapshot of key stats from one of the world's busiest centers

‘Sac flow’ is more precise and will ease unfounded patient concerns, experts argue

Join us in New York Dec. 4-5 for evidence-based instruction with real-world examples

Consensus statement outlines the team, infrastructure and experience needed to deliver TTVI safely and effectively