Locations:

Struma ovarii can give rise to uncommon malignancy
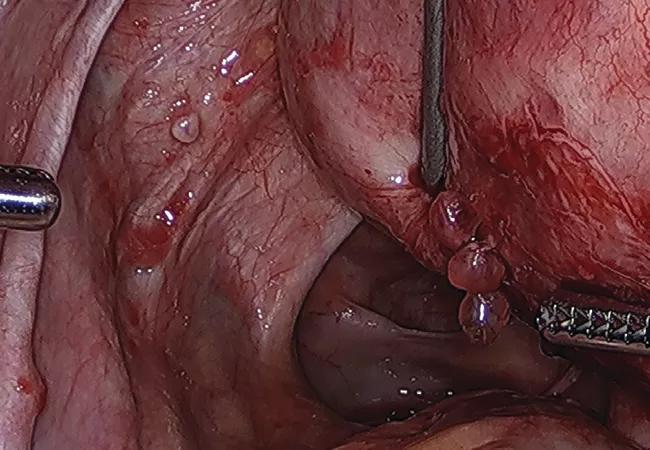
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/69ec2771-debd-4c65-a343-e01c9df517f1/22-WHI-3260168-CQD-HighlyDiffFollThy650x450hero_jpg)
struma ovarii thyroid carcinoma
Above, papillary lesions scattered throughout the left ovarian fossa and posterior uterus.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Cleveland Clinic doctors were preparing for a laparoscopic hysterectomy on a patient with an 11-centimeter uterine myoma when they noticed nodules on the fundus and anterior and posterior pelvic compartments. The nodules resembled endometriosis, but had a distinct appearance.
“They were round and looked a little bit more cystic,” says Miguel Luna, MD, Director of Endometriosis at Cleveland Clinic’s Ob/Gyn & Women’s Health Institute. “And they were clustered in a way we don’t generally see with endometriosis.”
Examination of a frozen tissue sample suggested the presence of a tumor of suspected thyroid origin. Instead of the hysterectomy, the surgical team performed right salpingectomy, peritoneal biopsies and pelvic washings. The eventual diagnosis was differentiated follicular thyroid carcinoma.
The health system’s multidisciplinary tumor board reviewed the case and, in partnership with the patient, charted a more extensive treatment course than originally had been planned: abdominal hysterectomy, right oophorectomy resection of left gonadal vessels, lymph node dissection, omentectomy and appendectomy. Follicular thyroid carcinoma was found on the uterine serosa, right ovary, left infundibulopelvic ligament and pelvic sidewalls.
The case illustrates the importance of having experienced team members in place who can detect subtleties that might otherwise be missed, says Dr. Luna. It also is a reminder to “trust your gut,” he adds, when something doesn’t seem quite right.
“Send a portion of whatever doesn’t look right to pathology as a frozen section, if you have that capability,” says Dr. Luna. “It is rare that we are in a position to pick up on these things, but when we are, we can keep the patient from having the wrong treatment.”
Advertisement
In this case, the patient had undergone left salpingo-oophorectomy three years earlier for removal of a struma ovarii – a germ-cell cyst that contains at least 50% thyroid tissue. While struma ovarii usually are benign, about 10% are malignant and classified as thyroid cancer. The patient’s cyst had been drained and removed without a specimen collection bag, which poses a risk for tissue spread.
“When you’re doing cystectomies, it’s very important to know that teratomas tend to leak,” says Dr. Luna. “Try to contain it as much as possible. Put a bag under it so that it doesn’t spill everywhere. And we always state in our training that when we have spillage from a teratoma, we irrigate the pelvis with about three liters of fluid to avoid tissue implantation.”
Struma ovarii are often asymptomatic and discovered incidentally. Thyroid carcinoma arising from germ cell tissue can happen independent of the health of the thyroid gland. Treatment recommendations vary depending on the severity of the disease. In the case of the 43-year-old, post-surgical adjuvant treatment was not recommended. She is being monitored and is doing well.
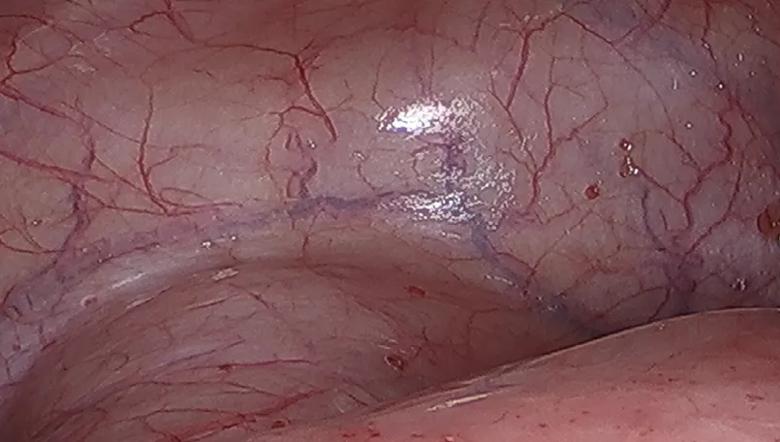
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/af6e04f1-2781-4fc1-b443-b3b23c7a4854/22-WHI-3260168-CQD-HighlyDiffFollThy805x456inset1_jpg)
Papillary red lesions were scattered throughout the anterior compartment of the pelvis.
Images are republished from The Journal of Minimally Invasive Gynecology, Vol. 29, Issue10, P1127-1128, Oct. 1, 2022, M. Luna Russo , M.S. Orlando, C. King, “Highly Differentiated Follicular Thyroid Carcinoma Arising from Struma Ovarii at the Time of Hysterectomy,” with permission from Elsevier.
Advertisement
Advertisement

Studies find mTOR inhibitor may play key role in treating Hurthle cell carcinoma

Dynamic risk assessment may aid clinicians in helping support informed treatment decisions
A new study indicates that the combined approaches can be performed without mortality and with acceptable morbidity

New research provides clinical insight into prognostic factors

The drug does not provide lasting disease control for most patients

A review of pathophysiology, risk factors, clinical presentation and treatment options
Only 33% of patients have long-term improvement after treatment

OMT may be right for some with Graves’ eye disease