Locations:

Collaboration includes clinical validation of predictive modeling tool, development of second-generation tool
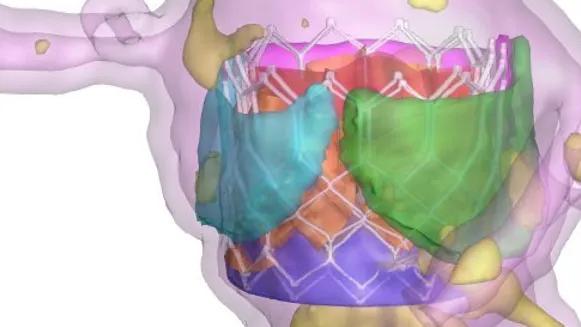
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a0b981b8-e37e-4dc0-ac5e-17eeb25d3d3e/precision-tavr-cqd-hero)
colorful imaging model of a heart valve procedure
Cleveland Clinic has partnered with the biomedical technology company DASI Simulations LLC to further validate the company’s predictive modeling technology for simulating transcatheter aortic valve replacement (TAVR) procedures. A second stage of the collaboration involves co-development of a second-generation tool for intraprocedural TAVR guidance.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
By combining Cleveland Clinic’s extensive clinical data and expertise with DASI’s artificial intelligence (AI)-powered simulation models, the partnership seeks to elevate the standard of TAVR care and improve long-term patient outcomes.
“Artificial intelligence is becoming a very important tool for procedural planning in structural cardiology,” says Samir Kapadia, MD, Chair of Cardiovascular Medicine at Cleveland Clinic and an interventional cardiologist who has been instrumental in TAVR’s clinical evolution. “Our work with DASI Simulations is aimed at clinically validating the use of their technology for TAVR planning and then breaking new ground by using AI for execution of the TAVR procedure rather than just procedural planning.”
The DASI technology allows physicians to visually simulate the transcatheter heart valve type and size within a patient’s specific anatomy prior to a TAVR procedure.
“High-quality imaging is the foundation of every successful structural heart intervention, and predictive simulation has the potential to further refine how we tailor procedures to individual patients,” notes Serge Harb, MD, of Cleveland Clinic’s Section of Cardiovascular Imaging. “By integrating detailed CT-derived anatomy with AI-driven modeling, DASI technology can help physicians better anticipate TAVR-related procedural challenges and optimize device selection and implantation strategy.”
While the software is already used by various centers across the nation, Cleveland Clinic’s initial role in the partnership involves a rigorous validation process at a high-volume expert center.
Advertisement
“We are currently using the software’s suggestions alongside our long-standing TAVR planning practices and measurements to assess for any differences,” Dr. Kapadia explains. He notes that this process, which began in late 2025 and is expected to last six months to a year, may result in recommendations on how the software’s outputs or data presentations might be adjusted for greater clinical utility.
Structural interventionalist Grant Reed, MD, MSc, is among the leading users of DASI technology for this validation exercise. “I continue to do my own measurements in planning TAVR cases, but I use the simulation as a confirmatory additional layer of support,” he says.
Dr. Reed notes that the value of predictive modeling lies in its ability to clarify complex anatomical relationships that are often difficult to visualize on standard CT reconstructions. He identifies the following as key clinical applications of the tool:
Advertisement
“Predictive modeling is all about simplification and personalization of TAVR planning, as it offers recommendations tailored to each patient’s anatomy,” Dr. Reed says. “We now have a DASI report generated for all our TAVR patients, and we review those reports individually and then also collectively at our heart team meetings. There have been instances where the simulation has prompted us to change care for patients, particularly when weighing TAVR versus surgery in the context of trying to envision optimal lifetime management for a given patient.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c2a8393d-b9a5-4bed-9b46-d29d7b12f10f/precision-tavr-cqd-inset)
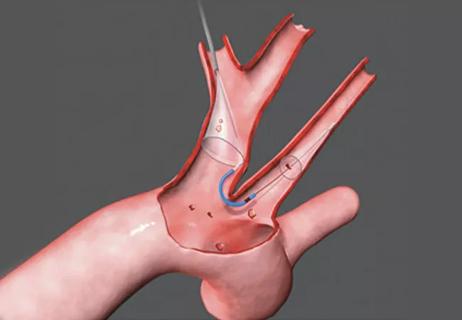
Examples of simulations generated by the DASI Simulations modeling tool for planning a basic TAVR procedure (left), a TAV-in-TAV procedure (middle) and a valve-in-valve TAVR procedure (right).
Cleveland Clinic believes that refining the tool and expanding the scope of its use will help broadly optimize TAVR care, enabling lower-volume centers to better replicate the quality of higher-volume centers.
While the partnership with DASI Simulations is currently focused on the aortic valve, it could potentially expand to the broader landscape of structural heart disease. Future applications might include predictive modeling for mitral and tricuspid valve procedures, Dr. Kapadia says, to extend similar AI-driven guidance to some of the most complex challenges in valve disease.
“We look forward to deepening our experience with the DASI modeling tool and learning how it can further contribute to procedural planning,” adds James Yun, MD, PhD, a Cleveland Clinic cardiothoracic surgeon with a specialty interest in TAVR. “The future potential for this and other AI tools to enhance both the planning and execution of both percutaneous and open surgical procedures is exciting.”
Advertisement
Disclosure. In addition to this partnership, Cleveland Clinic is an investor in DASI Simulations and may benefit financially from the sale of this technology.
Advertisement
Advertisement

TVT Registry analysis could expand indication to lower surgical risk levels

Patient series and bench validation support efficacy and safety of CLEVE procedure

In the wake of NOTION-3 findings, a strong argument for physician judgment remains
Post hoc analysis of PROTECTED TAVR finds reduced stroke risk in the U.S. but not beyond

Analysis of STS/ACC TVT Registry finds greatest benefit in patients with prior stroke

TAVR explant demands multidisciplinary expertise

How our HVTI Advisory Services team facilitated swift improvements for an allied health organization
Support for a TAVR-first approach in patients with concurrent valve and coronary disease