Locations:

TAVR explant demands multidisciplinary expertise
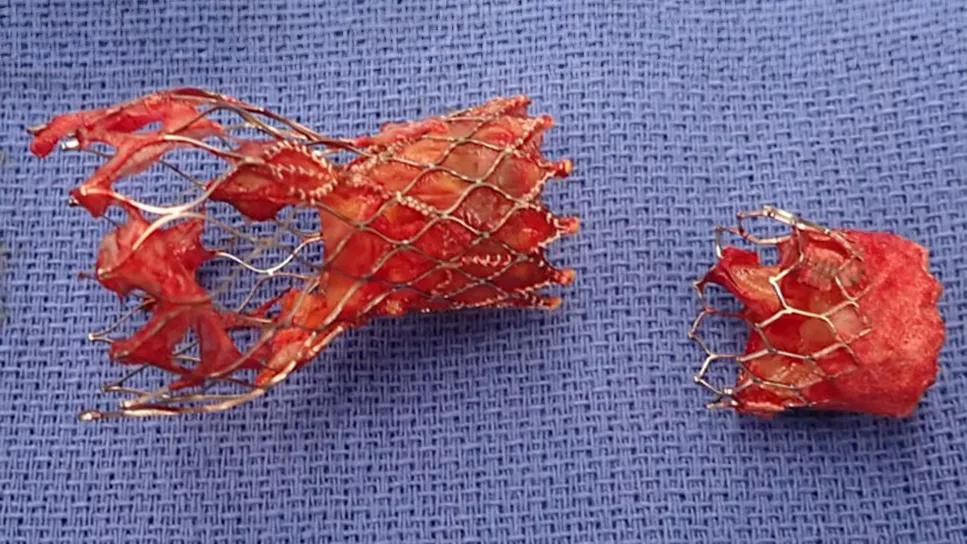
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e18182d5-6f19-4439-846f-cf42efc5bf34/tavr-explant-feature)
explanted TAVR prosthesis
All bioprosthetic valves, whether placed by surgical or transcatheter insertion, have a specific lifespan. While explantation of surgical aortic valves has been safely performed for many decades, removing transcatheter aortic valve replacement (TAVR) valves is a recent development that carries increased risk.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 2022 Cleveland Clinic study of 59 consecutive patients who underwent cardiac surgery after TAVR revealed that 78% of the operations involved TAVR explantation (Ann Thoracic Surg. 2022;114:52-60). Moreover, the study found that the interval between TAVR implantation and explantation decreased substantially over the course of the study period, which ran from 2012 to 2020.
The Cleveland Clinic cardiac surgeons behind this research have updated data for publication, and they say the trend of more and earlier TAVR explantations has continued. Their research includes analysis of the trend, which they attribute largely to inappropriate patient selection, patient-prosthesis mismatch, infective endocarditis or failure to address concurrent problems, such as coronary artery disease or mitral valve disease.
“TAVR was initially developed as an alternative to surgical aortic valve replacement (SAVR) in patients at high to medium risk from surgery,” says Marijan Koprivanac, MD, MS, a Cleveland Clinic cardiac surgeon specializing in aorta and aortic valve surgery. “As indications have expanded to include low-risk patients, a significant percentage of TAVR recipients are now younger and healthier. They love the option of a less-invasive procedure that allows them to go home the next day, but these patients are likely to outlive their replacement valves, whether they be TAVR or SAVR valves. Heart teams should fully consider patients’ long-term needs when deciding between SAVR and TAVR for initial valve replacement, with an eye toward potential future replacement procedures. One approach may set the stage for future procedures better than the other, but this is often determined on a case-by-case basis after factoring in patient age, overall health, life expectancy and specific anatomic considerations usually based on CT imaging. It really is an individualized decision that requires a heart team approach and shared decision-making with the patient.”
Advertisement
Today’s TAVR valves may last 10 years or more, but long-term durability is unknown and longer-term follow-up will be needed. Reasons for TAVR prosthesis failure include stenosis/regurgitation, paravalvular leak and endocarditis. Further, some patients may require cardiac surgery after TAVR for another reason, even if the TAVR valve is still working properly, in which case the TAVR valve is often still explanted and replaced with a surgical bioprosthesis.
When a TAVR valve needs to be replaced, the options are insertion of a second valve inside the first (valve-in-valve TAVR) or surgical explantation followed by SAVR. In cases where endocarditis is present, the infected tissue must be removed, making SAVR the sole option.
Dr. Koprivanac considers SAVR to generally be the better treatment option for a failing TAVR valve in many patients at lower surgical risk. “With valve-in-valve TAVR, the second valve makes the annulus smaller and creates a higher pressure gradient, so it is not ideal in many cases and is not possible in others,” he says.
“Valve-in-valve TAVR is also a great option when the initial TAVR is a large valve and there is appropriate space around it,” notes Amar Krishnaswamy, MD, Section Head of Interventional Cardiology. “The same considerations regarding sizing need to be made when placing a SAVR valve. That is why it is vitally important that a multidisciplinary team with expertise in surgery and transcatheter treatment works together to provide the best option for each patient.”
Advertisement
Dr. Koprivanac says there is growing evidence that, in general, when SAVR follows TAVR, outcomes tend to be worse than when TAVR follows SAVR. “In most cases, the intervention sequence should be planned so that TAVR is the last intervention,” he says. “SAVR can provide an ideal foundation for valve-in-valve TAVR.”
When infective endocarditis develops in a TAVR prosthesis, there is no question about treatment. “The valve must be removed, along with all traces of infection,” says Haytham Elgharably, MD, Surgical Director of Cleveland Clinic’s Endocarditis Center.
“Explantation can be complex, especially if the surgeon does not do a large number of aortic root procedures,” he continues. “A high-volume center like Cleveland Clinic can handle the pathology and avoid destroying the root.”
“The good news,” adds Samir Kapadia, MD, an interventional cardiologist and Chair of Cardiovascular Medicine, “is that the risk of endocarditis is similar in trials that compare TAVR and SAVR, so it does not appear that TAVR itself increases endocarditis risk.”
Dr. Elgharably notes that the explant procedure generally carries a high mortality rate, citing a 2021 report from the EXPLANT-TAVR international registry detailing outcomes of 269 TAVR patients undergoing TAVR explantation at 42 centers (JACC Cardiovasc Interv. 2021;14[18]:1978-1991): 30-day mortality was 13.1%, and 54.6% of patients required a concomitant cardiac procedure. Importantly, most patients in this series were elderly and at a high level of surgical risk, not a low-risk surgery population, which limits how broadly these data can be extrapolated.
Advertisement
At Cleveland Clinic, patients with symptoms of TAVR failure are examined with transthoracic echocardiography. If the findings suggest a problem, transesophageal echocardiography (TEE) and/or cardiac computed tomography (CT) may be done.
"These are complementary tools,” says cardiologist Serge Harb, MD, of the Section of Cardiovascular Imaging. “Both have excellent spatial resolution. TEE also has excellent temporal resolution, so we use it to assess the valve leaflets and to determine the severity of valve dysfunction. CT provides excellent anatomic definition of the valve and its surrounding area, and it also helps in planning potential interventions.”

Image content: This image is available to view online.
View image online ( https://assets.clevelandclinic.org/transform/97d80f87-4287-4e0b-92d2-4c1c76b2af41/tavr-explant-echocardiogram)
A transesophageal echocardiogram from a patient with complex infective endocarditis involving a TAVR prosthesis. The coexistent abscess, fistula and vegetation illustrate the complexity of cases like these.
Not uncommonly, a patient with suspected endocarditis may present with recurrent positive cultures but with no visible vegetation on echocardiography and perhaps just thickening of the leaflets. Without a clear diagnosis of endocarditis on initial imaging, some cardiologists hesitate to refer and will start the patient on antibiotics. Dr. Elgharably discourages this practice.
“These patients should be referred to a specialized endocarditis center,” he says, “as they may need specialized imaging for diagnosis, such as a PET scan. If endocarditis is present in the prosthetic valve, explanting the prosthesis is the only way to cure the infection. However, if the patient is at prohibitive risk for surgical extraction (as some TAVR patients are), they will need antibiotics indefinitely. If you stop the treatment, the infection will get worse.”
Advertisement
“If there is an infection extending from the valve to the aortic root, CT can define the extent of the problem,” Dr. Harb adds.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4909f330-74cf-4fa1-a1d9-e278fd7fb5b7/tavr-explant-1)
Explanted Evolut and Sapien TAVR valves from the same patient. The Sapien valve, which lasted one year, was placed into the Evolut valve after the latter showed early deterioration after three years.
As a major referral center for complex valve replacements and endocarditis surgery, Cleveland Clinic sees the results of less-than-successful attempts at treating failing TAVR valves. One case, recently published by Dr. Elgharably and colleagues in the Annals of Thoracic Surgery (2023;1[2]:316), was marked by TAVR valve embolization to the aortic arch. Instead of removal, a second TAVR valve was implanted, but residual paravalvular leak was detected. Failing to find relief from symptoms, the patient sought treatment at Cleveland Clinic, where both prostheses were carefully removed and successful SAVR was performed.
Such cases underscore recommendations that TAVR explantation be performed only by a team with experience and expertise in valve replacement, aorta and aortic root surgery, multimodality imaging and endocarditis.
“The aorta grows into the nitinol cage, and it is easy to damage the aorta when peeling it away from the prosthesis,” Dr. Koprivanac notes. “In addition to replacing the valve, the surgeon must be prepared to replace the aortic root and repair or replace the ascending aorta as well.
“TAVR is unquestionably a fantastic development,” he continues, “but in those cases when an implanted TAVR valve is failing, referral to a center with high volume-based experience in TAVR explantation can mitigate some of the risk inherent to this increasingly frequent presentation.”
Advertisement

Collaboration includes clinical validation of predictive modeling tool, development of second-generation tool

TVT Registry analysis could expand indication to lower surgical risk levels

Patient series and bench validation support efficacy and safety of CLEVE procedure

In the wake of NOTION-3 findings, a strong argument for physician judgment remains
Post hoc analysis of PROTECTED TAVR finds reduced stroke risk in the U.S. but not beyond

Analysis of STS/ACC TVT Registry finds greatest benefit in patients with prior stroke

How our HVTI Advisory Services team facilitated swift improvements for an allied health organization
Support for a TAVR-first approach in patients with concurrent valve and coronary disease