Locations:

Guidance from an expert on distinguishing — and co-managing — the disorders

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/11aa90ac-8d66-4d23-b96d-f077c03ff540/24-NEU-4568961-CQD-Hero-967x544-1_jpg)
photo of woman looking anxious on a couch
The chances of success in treating postural orthostatic tachycardia syndrome (POTS) are reduced among patients who also carry a diagnosis of anxiety, new Cleveland Clinic research suggests.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In an analysis of electronic medical records for 322 patients with a confirmed diagnosis of POTS seen at Cleveland Clinic’s tertiary referral center between 2018 and 2022, two-thirds also had a diagnosis of anxiety disorder. After adjustment for confounding factors, the individuals with anxiety were 2.6 times as likely to have had at least one change in their POTS treatment. The study was published in General Hospital Psychiatry.
“We found that if patients had a coexisting diagnosis of anxiety, that led to more POTS treatment failures,” says senior investigator Robert Wilson, DO, a neurologist in Cleveland Clinic’s Neuromuscular Center. “This may be a more challenging group to treat.”
POTS is a heterogeneous and often debilitating condition affecting the autonomic nervous system, estimated to affect between 0.3% and 1% of the U.S. population. Its incidence is believed to be rising among people with a prior COVID-19 infection, as a likely component of so-called long COVID.
The condition is characterized by chronic orthostatic intolerance and an excessive increased heart rate upon standing. Other symptoms include fatigue, headaches, cognitive impairment, palpitations, chest pain and gastrointestinal symptoms. These symptoms can significantly reduce quality of life and may lead to job and income loss.
Clinicians should recognize the major adverse impact that POTS can have on a person’s life, particularly for young patients (most people with POTS are under age 50), and the possibility that this can lead to concurrent mental health conditions, Dr. Wilson says.
Advertisement
“People with POTS have tremendous upheaval in their lives,” he notes. “Their social drivers of health may be impacted, which can lead to anxiety. Anxiety disorders may be developing without being addressed. Clinicians may be focusing just on POTS and not adequately assessing the broader impact of this syndrome. There needs to be a much more comprehensive, holistic review of these patients’ lives.”
Many patients also experience delays in care, as it can take six to eight years to get an accurate diagnosis of POTS, he adds.
There is no single universally successful treatment for POTS, and no standard treatment algorithm. Most patients require a combination of pharmacotherapy, lifestyle changes and physical therapy.
“Treatment of POTS is challenging,” Dr. Wilson explains. “What we’ve shown is that the medications used to raise blood pressure, such as beta-blockers, fludrocortisone, and pyridostigmine, are less effective in patients with anxiety. We clearly need better treatments.”
Distinguishing between POTS and anxiety can be difficult, as some of the “hyper-adrenergic” symptoms of POTS — including tachycardia, palpitations, sweating and lightheadedness — can appear very similar to symptoms experienced by people with an anxiety disorder.
However, studies have demonstrated that the orthostatic tachycardia seen in POTS is not merely the somatization of anxiety. “It’s possible that many of these patients have a high sympathetic response that may be labeled as anxiety when it’s really POTS,” Dr. Wilson notes.
Advertisement
But if individuals with POTS later develop anxiety secondary to having a chronic medical condition, “they may have already been to many medical providers who have told them it’s psychiatric,” he says. “And once they get the POTS diagnosis, there could be resistance to the anxiety diagnosis.”
The difficulty in distinguishing between POTS and anxiety symptoms may be just one factor leading to POTS treatment failure among those with concurrent anxiety. Other contributors could include the underlying pathophysiology of anxiety disorders and the autonomic nervous system, the effects of pharmacologic anxiety treatments, and the effects of bias and stigma.
Dr. Wilson advises that clinicians use appropriate tools to differentiate POTS from anxiety. A tilt-table test is key in diagnosing POTS, while the two screening tools used in his group’s recent study, the Generalized Anxiety Disorder Assessment and the PROMIS Global Mental Health questionnaire, are helpful in screening for anxiety.
Further diagnostic follow-up is necessary after use of these screening tools, along with individualized care plans for one or both conditions. In all cases, Dr. Wilson says, “the results should lead to a conversation of where to go next.”
At Cleveland Clinic, patients with POTS receive multidisciplinary care, including from specialists in autonomic nervous system disease from neurology, psychology, cardiology, endocrinology, gastroenterology and sometimes other areas. “We have very integrated teams here,” Dr. Wilson says.
Advertisement
This paper is the first of several that the authors plan to publish on the effects of concurrent diagnoses — such as migraines and fibromyalgia — on the treatment of POTS.
Advertisement
Advertisement
For now, antibody testing is recommended only when considering an alternative diagnosis
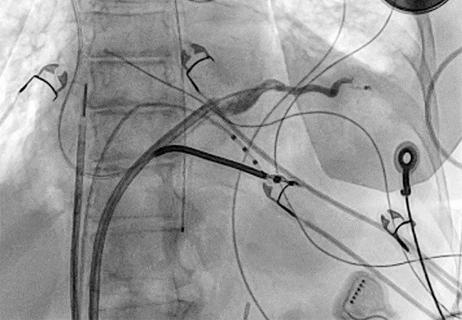
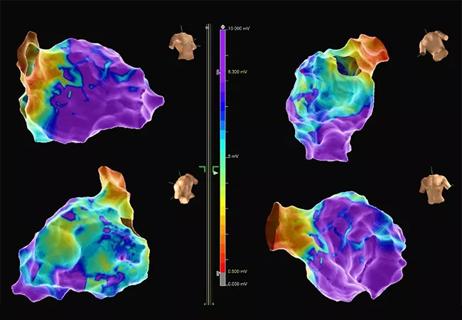
Procedure allows for safer epicardial VT mapping and ablation
Study finds that in the absence of ACS, the yield is low and outcomes are unaffected

Further study needed to assess potential role in select subgroups
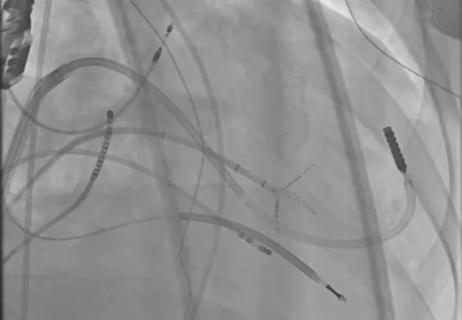
New technology aids a Cleveland Clinic London patient with a complex arrhythmia

Research shows promise for use in therapeutic settings to manage depression, PTSD, anxiety and more

Formal assessment aimed at unmasking psychological distress following PE treatment
After optimized medical and device therapy, is there a role for endocardial-epicardial VT ablation?