Locations:

Potential benefits include clinical guidance, TAVR outcome prediction, device testing

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f26a4802-1b04-4ded-838c-86c0c87489c0/23-HVI-3673794-CQD-Hero-1a_jpg)
medical device with inset image
A desktop-sized cardiac modeling system made of pliable, 3D-printed materials can be customized to accurately mimic the hydrodynamic characteristics of individual patients’ aortic stenosis (AS), ventricular remodeling and diastolic dysfunction. So reports a study published in Science Robotics by the Cleveland Clinic- and MIT-led team that developed the modeling system.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The soft robotic model consists of a flexible shell in the exact shape of a patient’s left ventricle (LV) and aorta and surrounded by “tunable” pneumatic sleeves that mimic the patient’s aortic valve lesions and loss of ventricular compliance as fluid circulates in the system.
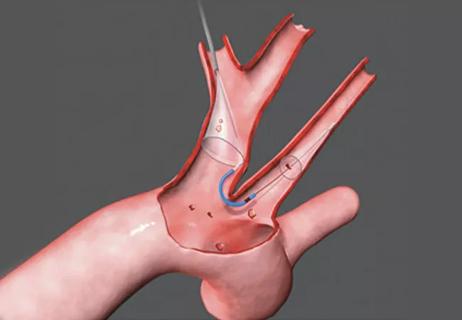
When a transcatheter aortic valve replacement (TAVR) prosthesis is implanted in an individualized model, the resulting hydrodynamic changes match the postoperative hemodynamics of the relevant patient fitted with a comparably sized TAVR valve.
The model’s ability to replicate patient-specific disease morphology and treatment outcomes builds on previous research by the Cleveland Clinic/MIT team published in Nature Biomedical Engineering. The findings lay the groundwork for eventual deployment of the technology to inform clinical decision-making for individual patients with AS and other cardiac conditions, as well as to predict treatment outcome and support the design, testing and selection of personalized medical devices.
“Development of a patient-specific, clinically relevant model of aortic stenosis is vitally important,” says the study’s co-senior author, Christopher Nguyen, PhD, Director of the Cardiovascular Innovation Research Center and Director of MRI Research in Cleveland Clinic’s Heart, Vascular & Thoracic Institute. “With further validation and testing, we hope to translate this research into an effective tool for clinical guidance, education and device evaluation.”
Despite significant advances in TAVR technology and technique, there remains a need for high-fidelity modeling approaches to predict prosthetic valves’ fit, functionality and hemodynamic performance, particularly for high-risk patients with complex anatomic or physiological conditions. Selection of an improperly sized valve can cause paravalvular leakage and other complications.
Advertisement
Current modeling platforms typically use synthetic valve leaflet materials and fixed-volume pulsatile pumping systems that may not reliably and accurately replicate disease-state, patient-specific hemodynamics and demonstrate treatment-associated changes. In addition, existing methods cannot simulate the diastolic dysfunction resulting from AS-related LV remodeling.
Dr. Nguyen and colleagues have worked to develop a more realistic, clinically relevant and customizable AS and ventricular remodeling simulator. They devised a soft, biomimetic robotic sleeve that encases and compresses the ascending aorta to mimic AS lesions arising from degenerative or congenital disease such as fused valve leaflets. Three inward-facing, inflatable pockets on the sleeve replicate the aortic valve’s trifold configuration (or that of a uni- or bicommissural valve if only one or two pockets are inflated). Thus, the sleeve can be tuned in real time to replicate patients’ aortic anatomies, unlike other models that must be iteratively tuned and reprinted or remanufactured.
Initial validation of a non-patient-specific aortic sleeve’s ability to recreate clinically relevant AS hemodynamics was conducted in a porcine model. The team subsequently developed a similar soft robotic LV sleeve that mimics loss of ventricular compliance and AS-associated diastolic dysfunction by the degree to which it is inflated, replicating impaired filling, emptying and wall motion during diastole and systole.
The researchers also used segmented CT imaging of selected AS patients’ left ventricles and aortas to create 3D digital anatomic models. The models were then 3D-printed using an elastomeric photopolymer resin to form soft, pliable, anatomically accurate cardiovascular shells.
Advertisement
By pairing an individualized ventricle/aorta shell with patient-specific, pneumatically tuned aortic and LV sleeves and circulating fluid through the system, the researchers could recreate the patient’s altered LV filling pressures, diastolic dysfunction and uniquely turbulent hemodynamics (Figure 1).
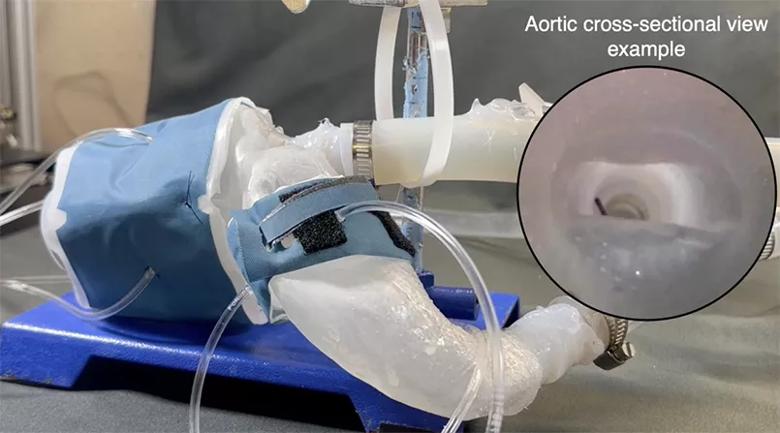
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/d0924be3-7480-43d6-8526-c8c53c38ce2c/23-HVI-3673794-CQD-Inset-1_jpg)
Figure 1. Representative 3D-printed left ventricle, aorta and aortic valve of a patient with aortic stenosis. The ventricle is driven by soft robotics mimicking the torsional motion of the heart and pumping blood out of the aorta, with the rest of the benchtop model connected to a mock flow loop matching a human body’s impedance.
“Current 3D printing methods create hard plastic cardiac models,” Dr. Nguyen says. “Our big leap was to make something that, although still synthetic, is close to the compliancy and response of the human cardiovascular system. The soft model allows you to determine whether the TAVR valve has the response desired when it deploys.”
To test the fidelity of their approach, Dr. Nguyen and colleagues created cardiac models representing 15 retrospectively chosen AS patients who had undergone transthoracic and/or transesophageal echocardiography as well as CT imaging for hemodynamic and anatomic AS evaluation. They compared each patient’s aortic valve cine CT imagery with the relevant robotic model’s aortic cross section under actuation of the aortic sleeve’s pockets as captured using an endoscopic camera.
They then compared critical hemodynamic parameters of AS measured in each patient — mean and maximum transaortic pressure gradients, peak aortic flow velocity and fluid volume ejected at each heartbeat — to the hydrodynamic values generated by the patient’s individualized model (Figure 2). The models replicated patient valve morphology and qualitative hemodynamic data with high accuracy in each case.
Advertisement
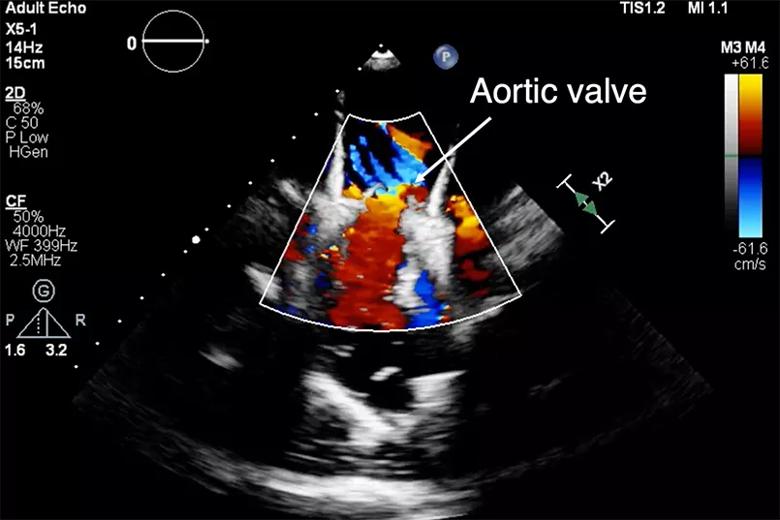
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/bff04c09-afb6-4932-a213-96cddc010f07/23-HVI-3673794-CQD-Inset-2_jpg)
Figure 2. Live hydrodynamic echo data across the 3D-printed model recapitulating flow through the aortic valve.
Next, in a subset of five patients, the investigators compared performance of their individualized soft robotic models to models containing aortic valves fabricated using a more conventional approach, with 3D-printed patient-specific aortic sinus and leaflet anatomies and rigid, calcium-like patterns corresponding to mineralized nodules. The soft robotic models more closely matched patients’ clinical parameters than did the models equipped with conventional leaflet valves.
To evaluate the ability of the model’s LV sleeve to mimic loss of ventricular compliance and diastolic dysfunction, the researchers tuned the sleeve’s actuation pressures to simulate the hemodynamics of four of the AS patients who had differing degrees of LV remodeling and had undergone LV catheterization. Again, the model was able to replicate measurements of the patients’ LV and aortic hemodynamics.
Finally, to test the system’s ability to predict the hemodynamic outcome of TAVR, the researchers compared postoperative clinical data from a subset of six patients with data from their individualized models implanted with comparably sized TAVR valves. Pre- and post-TAVR implantation measurements of transaortic pressure gradients showed high correlation between the models and actual patient readings.
“To be able to predict with the model what we see in a patient is clearly important,” Dr. Nguyen says. “If we don’t match what we get from our clinical data, the model will not be informative.”
Advertisement
Ultimately, Dr. Nguyen envisions a process in which medical imaging prior to TAVR is used to generate an individualized model that guides decisions about the correct valve size to implant and, perhaps, the creation of a customized valve.
“Our goal is to be able to perform a 3D scan and then create a subject-specific valve,” he says. “An accurate, high-fidelity model is the first step of many towards a personalized valve.”
“Despite incredible advancements in the TAVR arena, there remains a significant number of patients who cannot proceed with TAVR with the valves that are currently commercially available, due to unfavorable anatomy and/or areas of calcification,” says Deborah Kwon, MD, Director of Cardiac MRI at Cleveland Clinic. “However, this important advancement in valve disease simulation and modeling provides an essential platform that enables the possibility of personalized valve interventions and potential customized valve development. It will be exciting to see how this technology enables further innovation and advancement in TAVR care.”
Dr. Nguyen also foresees the model’s use in medical education and procedural planning. “You can think of it as another visualization tool, a way to help interventionalists learn how to approach a procedure in advance,” he says.
To achieve those goals, however, the modeling system will need further validation and eventual human clinical trials. In the near term, the team is focusing on developing a method to use MRI rather than CT imaging to generate the digital model of a patient’s heart, as well as speeding up the 3D printing process from that digital data.
Advertisement

Collaboration includes clinical validation of predictive modeling tool, development of second-generation tool

TVT Registry analysis could expand indication to lower surgical risk levels

Patient series and bench validation support efficacy and safety of CLEVE procedure

In the wake of NOTION-3 findings, a strong argument for physician judgment remains
Post hoc analysis of PROTECTED TAVR finds reduced stroke risk in the U.S. but not beyond

Analysis of STS/ACC TVT Registry finds greatest benefit in patients with prior stroke

TAVR explant demands multidisciplinary expertise

How our HVTI Advisory Services team facilitated swift improvements for an allied health organization