Locations:

Maintain a high index of clinical suspicion and consider the underlying etiology

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/87ced4c7-8e0a-4e75-a27b-1375d53a5683/woman-chest-pain-2263355856)
woman on a bed grasping her chest in front of a doctor
Although premenopausal women traditionally have been considered at lower risk of acute coronary syndrome (ACS) than other populations, myocardial infarction (MI) is being seen with increasing frequency in younger women.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Because premenopausal women with ACS may present differently than their postmenopausal counterparts and may not have a typical cause for their ACS, MI symptoms in younger women often are incorrectly attributed to noncardiac causes. Studies show that premenopausal women with ACS are less likely than men to undergo cardiac catheterization and revascularization and to receive guideline-directed medical therapy. Consequently, their outcomes tend to be worse, and mortality rates from MI are higher in younger women than in men of the same age.
To address this large clinical practice gap, the American Heart Association (AHA) commissioned ascientific statement on acute coronary syndrome in premenopausal women (Circulation. 2026;153[7]:e89-e108). The document provides diagnostic and holistic management pathways for physicians encountering young women who present with chest pain.
“There are no specific guidelines to direct physicians caring for young women with suspected ACS in the emergency department,” says Cleveland Clinic interventional cardiologist Jacqueline Tamis-Holland, MD, one of 10 authors of the scientific statement. “Our goal was to provide physicians with the information they need to diagnose the underlying disease and manage individual patients throughout their hospitalization and after discharge.”
The statement outlines six entities frequently reported as causes of ACS in women ages 65 and younger as well as four common conditions that mimic ACS. Rather than providing details on how these entities should be treated, it lays out the thought process physicians should follow when facing a premenopausal patient with ACS.
Advertisement
“A large proportion of premenopausal women with ACS have coronary artery disease due to atherosclerosis,” Dr. Tamis-Holland says. “Therefore, from the minute they enter the emergency department, premenopausal women with symptoms consistent with ischemia need to be treated with the same consideration as men.”
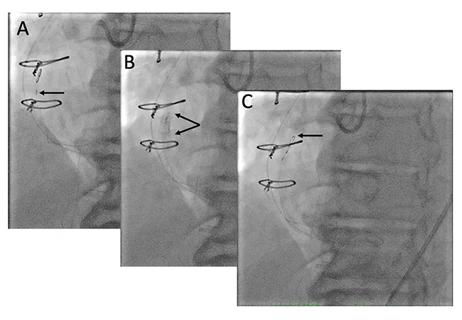
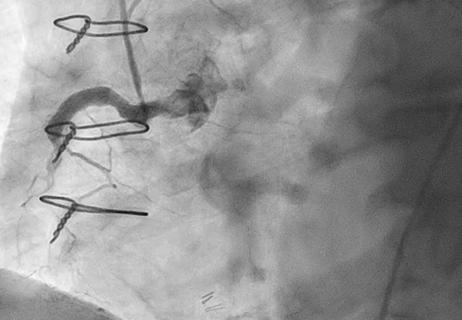
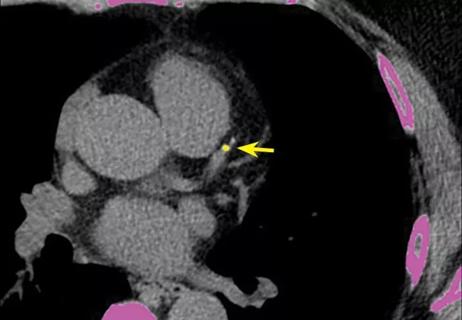
Simultaneously, physicians need to keep in mind that a significant proportion of these patients will have a condition other than atherosclerosis leading to their presentation. “When assessing a young female patient,” Dr. Tamis-Holland notes, “you also need to consider other possible etiologies, including spontaneous coronary artery dissection [SCAD], total occlusion of an artery from coronary embolism or other disease processes to explain the underlying cause of chest pain.”
Perhaps contrary to traditional medical training, young and female does not equate to low risk in contemporary acute cardiovascular care, adds cardiologist Amanda Vest, MBBS, Section Head of Heart Failure and Transplantation Cardiology at Cleveland Clinic.
“This important AHA statement certainly resonates with my experience on the cardiac intensive care unit, where it is not unusual to meet younger women diagnosed with ACS or even cardiogenic shock,” she says. “Any delays in recognition of ACS on the part of the patient or the clinician have the potential to hinder timely progression to coronary intervention or temporary mechanical support when indicated.”
The statement recommends that an ECG be taken within 10 minutes of the patient’s arrival in the emergency department. Troponin levels should be obtained with a high-sensitivity assay, if possible. At this point, any woman of childbearing age also should be tested for pregnancy to help guide decision-making.
Advertisement
Whether testing suggests an ST-elevation myocardial infarction or other entity, the statement authors agreed that the majority of women presenting with symptoms suggestive of ACS should undergo cardiac catheterization. “Irrespective of whether the patient is truly having an MI, coronary angiography helps clarify the issues to be addressed,” Dr. Tamis-Holland says.
The document outlines when coronary computed tomography angiography (CCTA) should be considered in lieu of coronary angiography and which tests to perform when ACS symptoms persist in a patient whose arteries appear normal on CCTA. It also explains when revascularization is needed for patients with SCAD or coronary artery disease.
“A key lesson in this statement is the value of institutional clinical protocols that facilitate prompt recognition and management of ACS and cardiogenic shock, including defined timepoints for troponin and lactate biomarker measurements and clear triggers for escalation of cardiac care,” says Dr. Vest.
After a diagnosis is made, the authors emphasize that the physician’s focus should shift to determining which tests and medical therapies are needed to mitigate future risk. “You need to be aggressive in assessing and treating risk factors in young women with coronary artery disease due to atherosclerosis, because they are at high risk,” Dr. Tamis-Holland says. “That’s why they have such extensive atherosclerosis at a young age.”
In addition to medications and lifestyle changes for traditional risk factors, the document suggests addressing other factors that could hinder recovery. This may include assessing the patient for depression and anxiety and determining whether they have supportive home conditions. Participation in cardiac rehabilitation should be strongly encouraged.
Advertisement
A highlight of the document is the consideration given to caring for pregnant women throughout the diagnostic, treatment and post-treatment processes. This includes the importance of consultation with obstetrics to discuss balancing the risk of radiation to the fetus with the benefits to the mother of invasive ACS management. The statement outlines guidance for shielding the fetus during catheterization and details which medications are likely to be absorbed into breast milk.
The new document is sufficiently detailed to be of value to any physician who takes emergency call or cares for patients with ACS. Nevertheless, the writing process revealed gaps in knowledge. The authors proposed 17 topics in six areas that need to be addressed, including medications and strategies to prevent recurrence.
Dr. Tamis-Holland notes that younger women with ACS traditionally have fared less well than younger men with the condition. One key unanswered question is whether differences in outcome would still exist if women were treated aggressively with contemporary management. “If sex-based differences in outcome persist even after equally aggressive care, the question remains what else we might do to improve outcomes,” she observes.
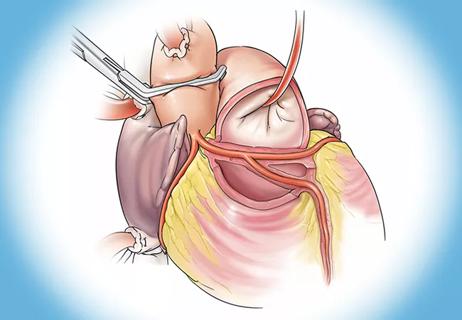
Another important question is whether percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) is the better treatment for women of any age with multivessel disease. A randomized clinical trial called RECHARGE (NCT06399692) is looking specifically at this issue. Cleveland Clinic hopes to begin enrolling patients this year.
Advertisement
“RECHARGE is looking at hard outcomes, not only MI and death, but also quality of life at one, five and 10 years,” Dr. Tamis-Holland says. “If PCI and CABG in women carry the same likelihood of success in terms of longevity, the question remains whether there are differences in quality of life that might favor one strategy over another.”
Dr. Tamis-Holland hopes physicians who adopt the thought process outlined in the new scientific statement will feel confident treating ACS in younger women.
“We need to have a high index of suspicion that premenopausal women with ACS have atherosclerotic disease or other conditions to explain the acute presentation,” she advises. “We need to be aggressive with care and be thoughtful about post-hospitalization care with cardiac rehabilitation, assessing for psychosocial risk factors such as depression and lack of a supportive home environment. We must aggressively treat women with atherosclerotic risk factors using medications and lifestyle modifications to prevent disease progression.”
Advertisement

5 biggest changes according to Cleveland Clinic experts
While procedural success rates lag overall, they shine for retrograde crossing
Lower success rates, more hospital MACE seen with poor-quality distal targets

Important additions to a novel surgical technique
Retrospective findings from an executive health program spur interest in broader studies
Growing awareness of impact leads to proliferation of procedures

Two research projects aim to enable more personalized MS care in this population

A reliable and reproducible alternative to conventional reimplantation and coronary unroofing