Locations:

A device implanted at the ankle joins the lineup of third-line treatments

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/d7f0af2d-65b1-47a2-9514-5121849376f9/overactive-bladder-2240867562)
Older woman sitting with hands on lower belly, looking uncomfortable
Urge urinary incontinence can be a debilitating condition. Patients experience sudden, frequent and overwhelming urges to urinate, and may experience leaking before they can reach a bathroom. A new implantable device can reduce those symptoms by automatically stimulating a nerve in the patient’s ankle, offering an alternative to medication and other therapies.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The device is implanted in the ankle and delivers painless stimulation to the tibial nerve three times a week. The stimulation helps suppress overactive sensory signals in the brain that tell the bladder it’s time to urinate. Studies have found that 80% of patients experienced improvement in their urinary symptoms with the device.
“The theory of tibial neuromodulation has been around for a long time, but these devices are newer,” says Amy Gee, MD, a Cleveland Clinic urogynecologist specializing in pelvic floor disorders. “This offers another option to patients who have overactive bladder.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/dbfa930a-2c52-43d0-8923-0b1f133c4228/altaviva-device)
(Image courtesy Medtronics)
Patients with overactive bladder may feel the urge to urinate as frequently as every one to two hours and may also experience urge incontinence. This can often be a result of aging, which can cause weakening of the brain’s ability to suppress the urge to urinate. Neurological conditions such as Parkinson’s disease also can cause overactive bladder.
Treatment typically takes a three-step approach. Patients are first told to try lifestyle changes and behavioral modifications, like urinating more frequently, managing fluid intake and avoiding irritants like caffeine and alcohol.
If that approach fails, medication may be offered. Newer drugs such as vibegron (Gemtesa) and mirabegron (Myrbetriq) seem to have fewer side effects than older therapies, but even the best medications have limited efficacy, and many patients experience only minor improvement, Dr. Gee says.
Current third-line treatments include bladder Botox, an in-office procedure in which Botox is injected directly into the bladder muscle, relaxing the muscle and allowing patients to hold urine for longer. While this approach can be effective, patients must return for injections every six months to maintain results, and Botox can become less effective over time, Dr. Gee noted.
Advertisement
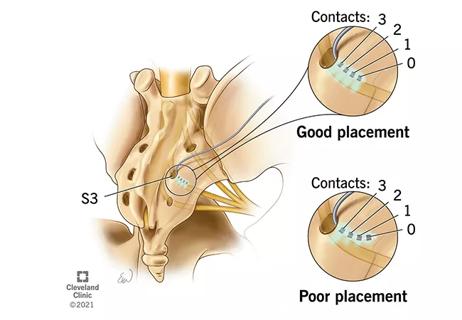
Another effective option is sacroneuromodulation via a device implanted in the upper buttock. This requires a trial period before the implant surgery, which is performed under general anesthesia. Some patients with lower back pain are wary of it because of the location, and some patients prefer a one-and-done procedure.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ca2a1306-c344-4452-aa3a-8097ca6effc1/tibial-stimulation)
Local anesthesia is used for the surgical implanation of the neurmodulation device. (Image courtesy Medtronics.)
The new tibial implant (AltivivaTM by Medtronics) received U.S. Food and Drug Administration approval in September 2025. Results are comparable to Botox and the sacroneuromodulation implant, Dr. Gee says, but some patients regard it as less invasive.
“The implant procedure takes less than 10 minutes and can be done under local anesthesia,” she says. “The device looks like a little USB stick. You literally just make a 2 cm incision on the inside of the ankle and slide it under the skin.”
The device is programmed using a remote control. Patients feel a slight tingling sensation during setup, which is done to confirm the device is placed correctly on the nerve. After that, the stimulator is set to a level that’s high enough to improve symptoms but low enough that the patient can’t feel it, Dr. Gee says. If the patient doesn’t notice an improvement in urinary frequency, the setting can be adjusted.
While the idea of tibial nerve stimulation has been around for a long time, other devices have been deigned to be administered at 30-minute sessions in-office every week.
“This is an update to that procedure, and it’s a way to make treatment more accessible for patients,” Dr. Gee says. “The patient doesn’t have to do anything. The device just delivers stimulation automatically.”
Advertisement
The tibial nerve branches off the sacral nerve, which connects to the bladder. It is thought that stimulating the nerve downregulates stray sensory inputs that signal the bladder to release.
“No one truly knows exactly how this works, we just know that it does,” Dr. Gee says. “We think this is kind of an electrical way of calming the signal down so that people are not getting all of those urges to go to the bathroom.”
Advertisement
Advertisement
Study leverages data from the ROSETTA trial
Could it unlock the potential for new approaches to treatment?

What it could mean for the future of ambulatory monitoring for bladder conditions

Nutrition and cooking program supports maternal-infant health

New moniker brings clarity to this complex condition

Aiming for earlier detection of endometrial cancer in an era of increasing incidence

Minimally invasive surgery is the preferred approach in many cases, but not all

Patients deserve timely diagnosis and a multidisciplinary approach